Electronic ISSN 2287-0237
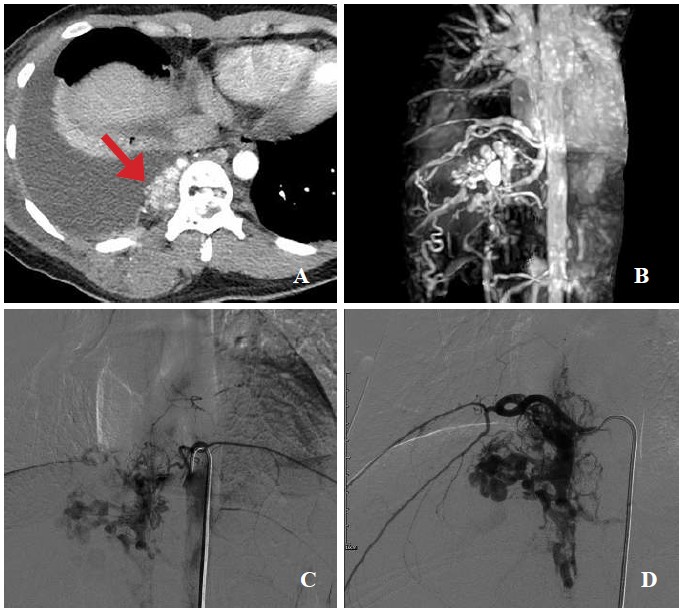
A 28-year-old Cambodian female patient presented with chronic cough and massive right pleural effusion. The pleuraleffusion was proven to be chylothorax. CT chest incidentally found a cluster of vascular malformation involving spinalcanal, vertebral bodies and paraspinal soft tissue at T9 to T12 levels (Fig. A). Spinal arteriovenous malformation waspresumably diagnosed. Further MR angiography of thoracic spine and conventional spinal angiography demonstratedarteriovenous fistula (AVF) at T9 level, fed via subcommissural branch of anterior spinal artery, and drained upwardly anddownwardly to perimedullary veins. Associated paraspinal arteriovenous malformation (AVM) along T9 to T12 levels wasnoted, fed via T9 to L1 intercostal arteries, later drainage to intercostal, paraspinal and azygos veins (Fig. B,C,D) Definitediagnosis was spinal arteriovenous metameric syndrome (SAMS) at T9 to T12 levels.
SAMS is a rare non-hereditary genetic metameric complex spinal vascular malformation, involving spinal cord and adjacentsoft tissue and/or bone in the same metameric level. Occurrence in female is more common than in males (2.5:1). The malformationsinclude arteriovenous fistula and nidus, the nidus form tending to be more complex and ruptured than the fistula one.Subarachnoid hemorrhage and hematomyelia are common presentations. The rate of second hemorrhage is up to 54%.Endovascular treatment is aimed at palliative prevention of a new episode of hemorrhage, occlusion and to stabilize themalformation.1









