Electronic ISSN 2287-0237
Greater accessibility within the ASEAN Community has led to more free movement of workers from various countries into Thailand, especially along the boundary lines of frontiers. The movement of people in these groups who enter Thailand for work, has both positive and negative aspects, especially with regards to public health. Sa Kaeo is the province with the largest movement of Cambodian migrant laborers who enter Thailand to work. There are more than 15,000 people entering the country per year in both the agricultural and industrial sectors1 and it has been found that maternal and child health is a major problem. The number of mothers and newborns admitted as inpatients has increased steadily from complications during pregnancy period until postpartum period because of inappropriate healthcare during pregnancy, being unaware of health care, nutritional deficiencies, high-risk work with low incomes, and theinconvenience of accessing health services. As a result, there is very little and delayed antenatal care and healthcare during pregnancy is inappropriate, as well as old cultural beliefs regarding pregnancy that may result in effects on pregnancy during pregnancy until postpartum period. Consequently, pregnant mothers are increasingly in need of hospitalization. The hospital cannot collect all payments from them, especially those who have no health insurance. Therefore, the hospital and the government to an increasing extent now bear the expense of Cambodian migrant laborers.1
From past studies of migrant workers, it was found that many migrant workers working in foreign countries faced many challenges such aspsychological stress, language barriers, housing problems, or difficulty adapting to a culture that is different from their home country.2-4 From the problem of adapting to a new culture that is different from the home culture and the different languages may cause an uncomfortable feeling when living in a new place, and when this adaptation occurs at the same time as pregnancy, it leads more and more to health problems or complications during pregnancy and postpartum. A proper healthcare behavior during pregnancy is important for migrant women to help prevent and to reduce the severity of health problems or complications, and to promote good health.5 In the provision of health promotion services aimed at pregnant women with different cultural backgrounds, it is necessary to know the specific factors that affect the health status of pregnant migrant workers in order to provide holistic care that is consistent with culture, beliefs, and lifestyles. Pender6 said that the promotion of health behavior consists of 6 aspects, such as the nutrition, health responsibility, exercise, interpersonal relationship, stress management, and spiritual development. People do change their healthcare behavior when they see that the change is beneficial to themselves. This is a result of individual experiences and a feeling that is specific to healthcare behavior which is consistent with their beliefs and culture.
From the literature review in the last 5-10 years, there are case studies on the factors influencing pregnant women’s healthcare behavior (PWHB), and mostly these studies are in Thai populations. However, there is no case study on the relationship between factors and Cambodian healthcare behaviors that migrate to Thailand. The opening up of the ASEAN Community allows for migrant workers to migrate into Thailand more freely. The majority of workers are in their reproductive age, resulting in higher pregnancy rates, approximately 10-20% delivery in each hospital.1 There are no clear reports to explore that the provision of health services for pregnant women with different beliefs and cultures from Thai culture may have factors that affect healthcare behaviors differently. Therefore, the appropriate service providers must understand the factors specific to the pregnant woman’s nationality, so that services can be modified to conform to the cultures, beliefs, lifestyles and behaviors of the pregnant women in question.
The researcher therefore was keen to study the factors for predicting the PWHB of Cambodian migrant laborers in Sa Kaeo province in order to provide basis data for creating a better understanding of factors that affect the healthcar behavior of this group of patients. This data can be used to provide an effective healthcare service to help reduce complications in pregnancy, the Bed Occupancy Rate and the burden of expenses to both hospital and government. The aim is to inform and improve the quality of healthcare service provided to Cambodian pregnant women on wards.
This study was descriptive research designed to study the predictive factors of pregnant women’s healthcare behavior of Cambodian migrant laborers who received antenatal care in public hospitals in the area of Sa Kaeo province. The data was collected from November 2016 to July 2017. Cambodian migrant laborers who were pregnant and who received antenatal care in public hospitals in area of Sa Kaeo province were studied. This study was approved by the Research Ethics Subcommittee Involving Humans, Thammasat University, 3rd Edition, Field of Science.
The inclusion criteria were:
antenatal care in public hospitals in the area of Sa Kaeo province.
Calculating the sample group size using the equation of n = 50 + 10k the result was 150, and the researcher increased the sample group by 20% to prevent data imperfection. So the sample group size for this study was 180 women.7
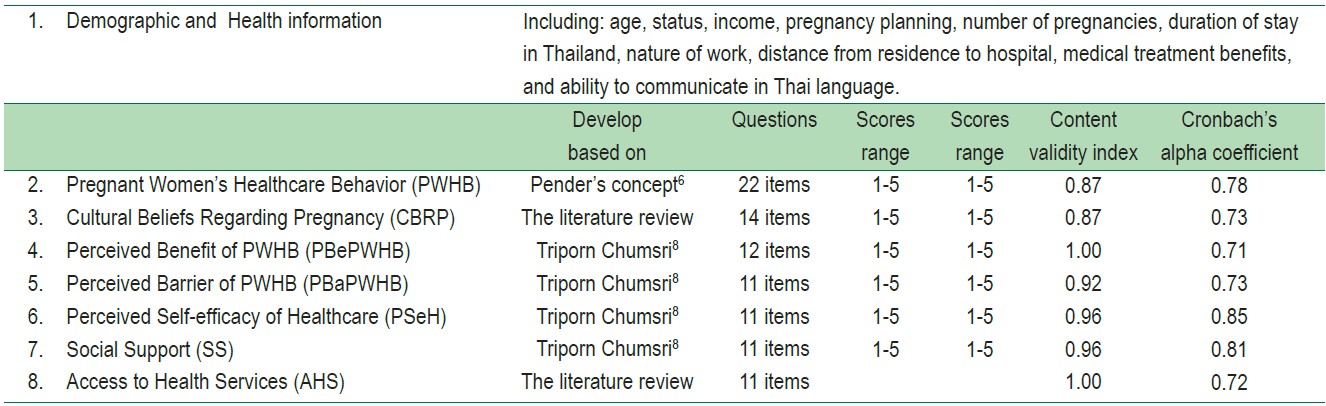
The research instruments were created in Thai before and translated into Cambodian using the back translation technique.7 The validity was verified by two Cambodian translators, a nurse and an obstetric doctor. The research instruments were interviewed questionnaires, with a reliability of Cronbach’s alpha coefficients at 0.71 and 0.85. The measures acquired accurate and identical texts by the obstetrics experts and Thai-Cambodian language experts. Information on the questionnaires used is expanded upon in Table 1 below.
Table 1 : Questionnaires used to study the behavior of pregnant migrant laborers.
Data Collection Method
The researcher started collecting data once the study passed the ethical criteria of research involving humans. The researcher met the participants at an appointed date and time and asked for cooperation in answering the interview form, providing the details of research, objective, benefit of research,protection of the rights of samples, data collection tools, and gave the opportunity to the participants to ask questions on the issue prior to signing the consent form for research. When the samples agreed to participate in the study, the research assistants began interviews by reading the interview formwhich took about 45-60 minutes. When the interview finished, the researcher checked the completeness and answered questions from the participants.
Data Analysis
Data was analyzed by using a statistical package program calculating the frequency, average, percentage, standard deviation, and relationship between variables by means of Pearson’s product moment correlation coefficient. The predictive factors of pregnant women’s healthcare behavior of Cambodian migrant laborers was analyzed with stepwise multiple regression analysis.
All of the 180 participants were aged between 14-40 years (26.30 ± 7.15) and about 80.60% were married. The average family monthly income was 6,541.67 baht (SD = 3,457.99).
Most women did not plan on falling pregnant, 83.30%, and late pregnancies accounted for 84.50%. Most of their work involved standing or walking, 58.30%. The journey from their residence to the nearest hospital took between 5 and 90 minutes (19.30 ± 0.14). The participants had been living in Thailand between 3 and 36 months (12.50 ± 7.79). Only 25.60% of them had health insurance. Nearly half of the participants were able to communicate in Thai at a basic level and 46.10% were unable to communicate in Thai at all. It was found that the overall average score was moderate (3.32 ± 0.22) when each aspect was considered separately, it was found that physical activity ranked the highest average score over other aspects (3.51 ± 0.58), the second ranked average was spiritual growth (3.25 ± 0.31), and stress management was ranked the lowest average score (2.59 ± 0.21).
It was found that cultural beliefs regarding pregnancy were negatively correlated with PWHB (r = -0.292, p <0.01) and the perceived benefit of behavior (r = 0.218, p < 0.01), as well as access to health services were positively correlated with the healthcare behavior of pregnant women with statistical significance (r = 0.201, p < 0.01), as shown in Table 2.
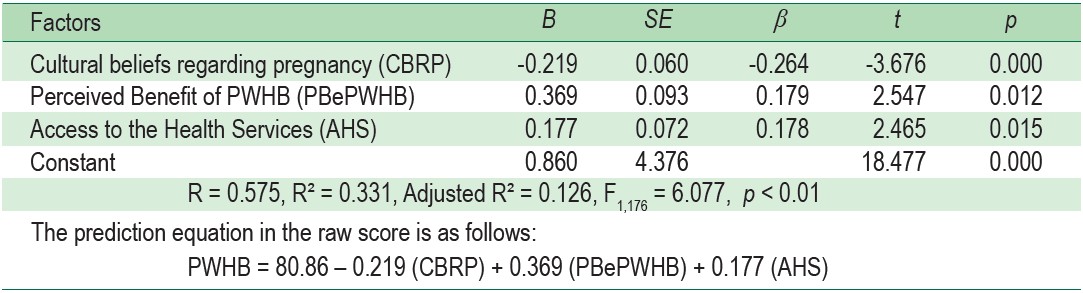
It was found that there were 3 factors that could explain the variance of PWHB scores with statistical significance at .01 level, these were cultural beliefs regarding pregnancy (β = - 0.264, p < 0.01), perceived benefits of behavior (β = 0.179, p < 0.05), and access to health services (β = 0.178, p < 0.05). All three factors could explain the variance of PWHB of Cambodian migrant laborers of 33.1% (R2 = 0.331, p < 0.01), as shown in Table 3.
Table 2 : Pearson’s product moment correlation coefficient of variables (n = 180)
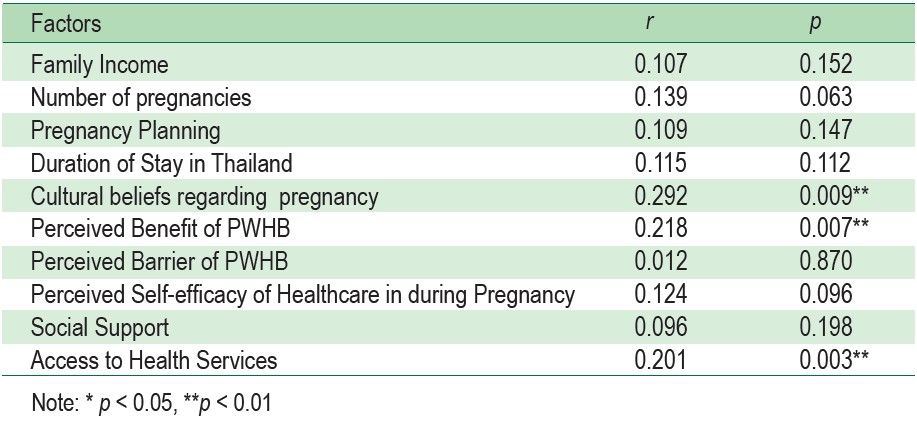
Table 3 : Predictive correlation coefficient of pregnant women’s healthcare behaviors of Cambodian migrant laborers (n = 180)
The overall level of PWHB of Cambodian migrant laborers was at a moderate level (3.31 ± 0.22). This might be due to the fact that more than 80% of the sample group had been pregnant before. In addition, participants who had visited an antenatal care clinic, might have received health education and become more aware about pregnancy, so these women may have had knowledge and experience in healthcare during pregnancy. Furthermore, the advantage of antenatal care would have been explained by a health professional as well as the sharing of knowledge about pregnancy. However, nearly half of the sample group (46.1%) was unable to communicate in Thai at all, therefore, they were not able to fully access knowledge and media produced in Thai. They would have had limited access to learn about self-care practices during pregnancy. What is more, the cultural belief of Cambodians is that being pregnant is a normal situation, so, antenatal care did not meet the criteria completely or antenatal care was not looked for near to giving birth. In addition, Cambodian pregnant migrant laborers had to work hard to earn their living, so, they had no time to practice healthcare behavior regularly during pregnancy, which was consistent with the study of Malaithong Wapee.9 This study researched pregnant women’s health promotion behavior in the Lao People’s Democratic Republic. The findings showed that the overall health promotion behaviors were moderate also (2.46 ± 0.45).
The cultural beliefs regarding pregnancy could predict the pregnant women’s healthcare behavior of Cambodian migrant laborers (β = -0.264, p < 0.01). The finding of this study was consistent with Pender’s health promotion concept6, which explained that cultural beliefs were the socio-cultural factors that directly affected health behavior practices. The cultural beliefs regarding pregnancy in each culture are the part of the experience and individual characteristics which affect the different healthcare behaviors according to their cultural beliefs. This study showed that the cultural beliefs regarding pregnancy could result in inappropriate healthcare behaviors during pregnancy such as drinking herbal solutions during pregnancy to promote good blood circulation. Or eating more than your husband will result in a big baby and a difficult birth. Also there was a belief that if you eat spicy food, the fetus will not grow, and there will be abdominal pain and diarrhea in a pregnant woman, and so on. This was consistent with a study of Thai pregnant women, which found that the beliefs about pregnancy correlated with pregnant women’s health promotion behaviors.8,10,11 In addition, a qualitative study found that the antenatal care of Cambodian pregnant women was low due to the cultural beliefs of Cambodians that believe in the super- natural and in folk medicine. They see the midwife as the caregiver during pregnancy, so, they thought that it was not necessary to get care from other medical providers.12
The perceived benefits of behavior could predict the pregnant women’s healthcare behaviors of Cambodian migrant laborers (β = 0.179, p < 0.05). The finding of this study was consistent with Pender’s health promotion concept6 that a person planning to practice a health behavior will depend on the benefits already received, which resulted in the positive way or positive reinforcement of those practices. This study showed that the sample group had high perceived benefits of healthcare behaviors and practices. As this helps select good behavior practical guidelines, the pregnant women followed the recommendations of health professionals to prevent hazardous potential complications, they chose to eat properly to make themselves and their fetus healthy. In addition, the finding of this study was consistent with the study of Malaithong Wapee9, which studied pregnant women in the Lao People’s Democratic Republic. There too, it was found that the perceived benefits positively correlated with pregnant women’s health promotion behaviors. In addition, the study on Thai pregnant women found that the perceived benefits positively correlated and could predict pregnant women’s healthcare behaviors.2,10, 13, 14
Access to health services could predict PWHB of Cambodian migrant laborers (β = 0.178, p <0.05), be consistent with Pender’s Health Promotion Concept,6 namely access to health services is affected by the context or influence of a situation. People’s perception and thoughts about a situation or context, could promote or hinder the practice of health promotion behavior. People prefer to choose the activities that make them feel in tune with their way of life and environment, as well as feeling safe and stable when practicing the promoted behavior in that environment. This study showed that the sample group can access health services. This might be given that the relevant health service facilities were not very far and could be reachedeasily. In addition, billboards in Cambodia’s official language made it simpler to understand the process or procedure of treatment. This finding is consistent with past studies showing that access to health services could predict antenatal care and care during the maternal postpartum period for pregnant women who migrated to Thailand (31.90% with a statistical significance of 0.05).14,15 A study by Wichuda Sankareak and colleagues,16 measuring the use of antenatal care service by migrant workers, found that the perception of antenatal care service usage by alien workers was the factor that led to a greater understanding of services provided and led to more appropriate healthcare behaviors.17,18
Our study indicates that there is moderate healthcare behavior among the Cambodian pregnant migrant laborers. The factors predicting the healthcare behaviors of Cambodian pregnant migrant laborers included cultural beliefs regarding pregnancy, perceived benefits of healthcare behaviors, andaccess to health services, which accounted for 33.1% of the variance. According to the findings, the health promotion activities of Cambodian pregnant migrant laborers should be aligned with cultural beliefs, must raise awareness of the benefit of healthcare behaviors, and should provide health services that Cambodian pregnant migrant laborers can easily access. In addition, the language barrier is a limitation for health care providers when working with Cambodian migrant laborers. It is essential to provide applicable health education techniques in Cambodia’s official language. This will ensure that this group of individuals will be able to access the full benefits good healthcare pregnancy behaviour.
The researcher would like to thank Thammasat University for its support and funding of this research and would like to thank the experts, and all of the sample group participants for their cooperation in this study.









