Electronic ISSN 2287-0237
Headache is a common presenting symptom for patients who visit neurologists at the neuroscience center in at the Bangkok Hospital Medical center. The statistics from the last 5 years show that headache was a presenting symptom in 65% of the patients. The comprehensive headache clinic has been established since 2011 in order to care for this group of patients more effectively.1, 2
The mission of the comprehensive headache clinic is to obtain standard diagnosis according to the International Classification of Headache Disorders 2nd Edition (ICHD-2)3 and to the holistic treatment guidelines from the American Academy of Neurology and the European Federation of Neurology Society. The clinical characteristics data on the severity of headache experienced by patients is very important to help identify the appropriate treatment plan.
The Headache Registry Program is a prospective study based on patient data from March to June 2013. The data collected included demographic data,characteristic of headache, diagnosis, treatment, clinical outcome, and treatment adherence.
Materials
The headache registry program consists of a headache registry questionnaire used to evaluate the patient’s experience of headache to include: a pain score assessment, the headache frequency per week, and a Migraine Disability Assessment Questionnaire (MIDAS). Once a detailed history has been collated and after the neurologist or headache specialist from the comprehensive headache clinic has completed their neurological examination, the patient will be diagnosed according to ICHD-2. Patients will then have an opportunity to discuss treatment strategies and to receive appropriate treatment consisting of headache education, trigger avoidance, pharmacological and non- pharmacological treatments on offer and also instructions in the use of a headache diary to document their symptoms and frequency of headaches.
The headache registry questionnaire is a questionnaire used to collate the patient’s history of headaches The questions cover the characteristics of headache, the duration, frequency and location of the headache, the pain score, any associated symptoms, trigger factors, and the impact the headache has on daily life, any history of past illnesses, and any medications used including analgesics.
A headache diary is used to record headache symptoms. The information includes the day the headache occurred, the pain intensity (pain score), duration, and triggers, any associated symptoms, and any analgesic used.
The pain score4 is a pain assessment graded on a numerical rating scale (NRS) ranging from a score of 0 to The scores are divided into 4 categories:
0 = no pain,
1 - 3 = mild pain,
4 - 6 = moderate pain
7 - 10 = severe pain.
The headache frequency per week is the number of headache attacks in a week.
The Migraine Disability Assessment Questionnaire (MIDAS)5-7 is a disability self-assessment tool for migraineurs. The questionnaire assesses the disability ranking in daily activities of migraine patients in 3 areas including work or study, household activity, and social activity for the previous 3 months. The results can be divided into 4 grades:
MIDAS Grade Definition MIDAS Score
Grade I Little or no disability 0-5
Grade II Mild disability 6-10
Grade III Moderate disability 11-20
Grade IV Severe disability 21+
Statistical Analysis
Methods
The data collection process is divided into 5 visits1:
• 1st Visit
Inclusion Criteria:
- Patients who are visiting the comprehensive headache clinic for the first time.
- Patients who have been diagnosed according to the ICHD-2 criteria as having primary head- ache disorder, secondary headache disorder, cranial neuralgias, central and primary facial pain, and other headaches.
- Patients aged 15 and above, who can communi-cate well.
Exclusion Criteria:
- Patients who declined taking part in the study.
- Patients whose diagnosis changed, and was not related to the ICHD-2 criteria.
• 2nd Visit (1-2 weeks), 3rd Visit (3-4 weeks), 4th Visit (5-9 weeks) and 5th Visit (10-14 weeks):
Population
Most patients are female (80%) with an average age of 36±11 years. The most common age range is 31-60 years (63%) followed by 15-30 years (34%) and > 60 years (3%).
The most common headache type is primary headache (82.9%), including migraine headache9 (68.6%) followed by tension type headache (11.4%) and other headaches (2.9%).
The second most common headache disorder is secondary headache (10.0%) including medication overuse headache (5.7%) and cervicogenic headache (4.3%). The least common type is cranial neuralgia, central and primary facial pain, and other headaches (7.1%) including occipital neuralgia (2.9%), tolosa-hunt syndrome (2.9%) and trigeminal neuralgia (1.3%). (Table 1)
Treatment
Medications for the treatment of headaches were divided into two groups: acute medications and prophylaxis medications.10-12 In acute medications, triptans were the most commonly used (59%), followed by non-steroidal anti-inflammatory drugs (NSAIDs) (41%). The most commonly used prophylaxis medications were antiepileptics drugs (48%), followed by antidepressants (45%) and calcium channel blockers (7%). (Figure 1)
Minor and transient adverse effects were found in 0.7% with acute medications and 16.22% with prophylaxis medications. Two patients (0.7%) experienced adverse effects after using triptans, including 1 case of chest pain and 1 case of nausea. There were 28 patients (13.16%) who experienced adverse effects after using tricyclics antide-pressants including 23 patients with drowsiness, 3 patients with dizziness, and 2 patients with constipation. Of the patients who took antiepileptic drugs, 4 patients (2.04%) had numbness in their extremities and 2 patients (1.02%) had memory difficulties. (Table 2)
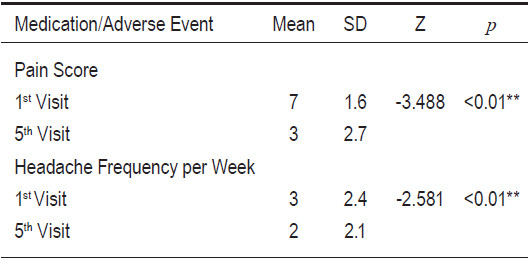
The average pain score dropped from 7 (severe pain) to 3 (mild pain) (Z = -3.488, p < 0.01). The average headache frequency per week was reduced from 3 to 2 times per week. (Table 3)
Table 1: Patient Characteristics (n=70).
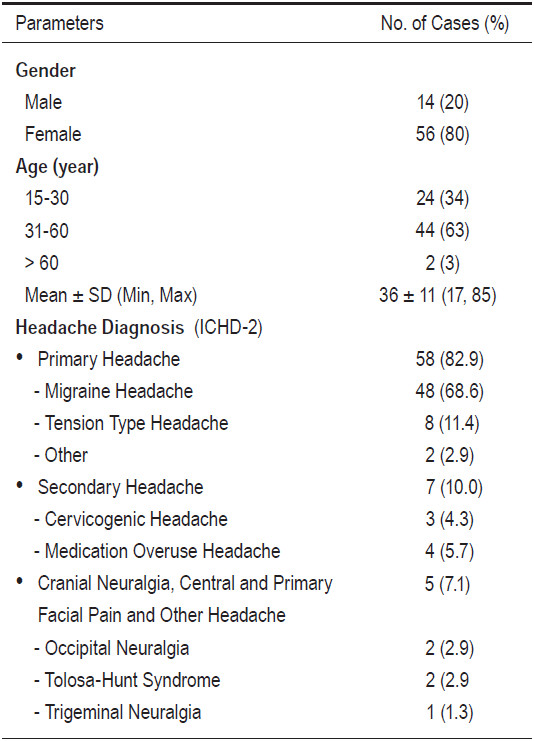
Table 2: Types and numbers of patients with side effects.
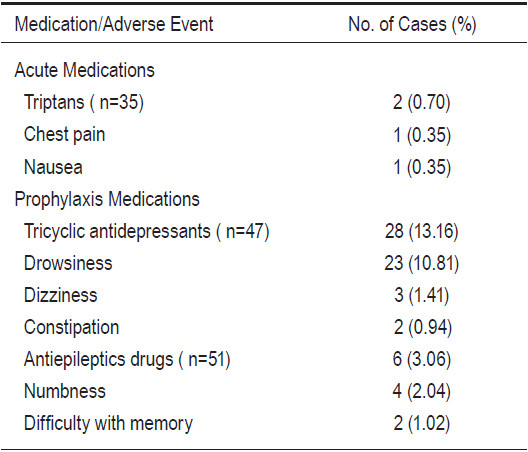
Table3: Headache parameters on 1st visit and 5th visit.
Patients’ Adherence
Patients’ adherence to treatment was evaluated as the percentage of patients that came to their appointment. Patients were divided into two groups according to their headache frequency as either episodic headache (head- ache frequency < 15 days per month) or chronic headache (headache frequency c 15 days per month).
Most of the patients with episodic headaches came to their 2nd visit (71.1%) and 3rd visit (65%), but most of these patients were not present at their 4th and 5th scheduled visit (11.1% and 0% respectively). The reason for not showing up for the appointment was evaluated via phone and it was found that 89% reported a dramatic improvement in symptoms, 8% were unavailable on the appointed date, and 3% were unreachable by phone.
Chronic headache patients scored a 100% attendance rate at the 1st, 2nd, 3rd, and 4th visit. However, 94.7% came to their 5th visit. The reason for not showing up for the appointment was also asked via phone, and the reason given was that the symptoms had improved and the follow-up visit was not seen as necessary.
Patients’ compliance to the medication was assessed by counting the leftover pills at each follow up visit. It was found that the compliance rate was 100%.
The results show that most patients who attended the comprehensive headache clinic suffered from migraine headache with a severe degree of symptoms (average pain score = 7, headache frequency per week = 3, MIDAS = 27.1). The first-line medication was triptans for acute treat- ment, and antiepileptic drugs for prophylaxis treatment. This is consistent with the guidelines from the American Academy of Neurology and the European Federation of Neurology Society.12-15
Most patients with episodic headache came in for follow-up during the first 2 visits, and when the symptomsimproved, most of these patients were not coming back for their later scheduled visits. Since none of these patients were present at the 5th visit, we could not compare the pain score, headache frequency per week, and MIDAS of the 1st versus 5th visit in this group. However, 63% of these patients said they would visit the comprehensive headache clinic should their symptoms relapse. This was a marked difference from their view prior to taking part in the program. Before, these patients would only have considered a visit to the clinic if their symptoms had been unbearable.
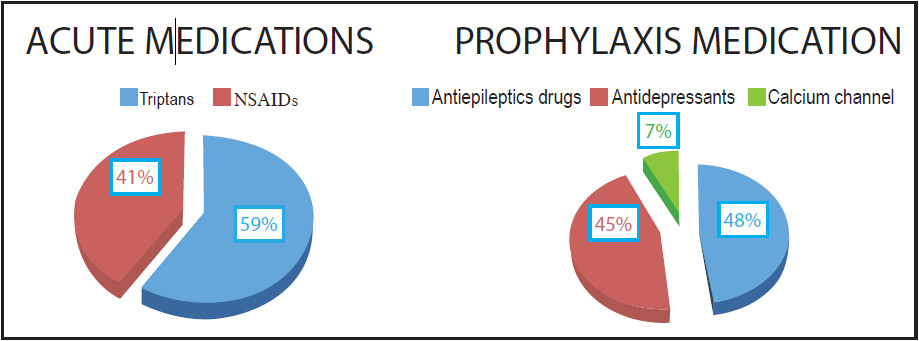
Figure 1: Medications used
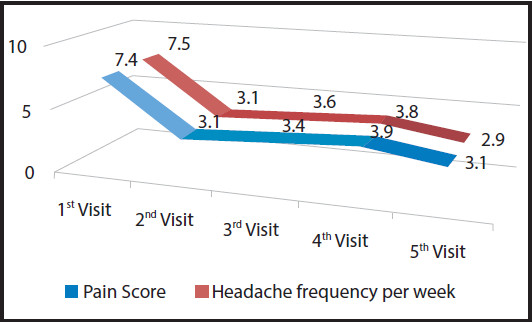
Figure 2: The average pain score and headache frequency per week
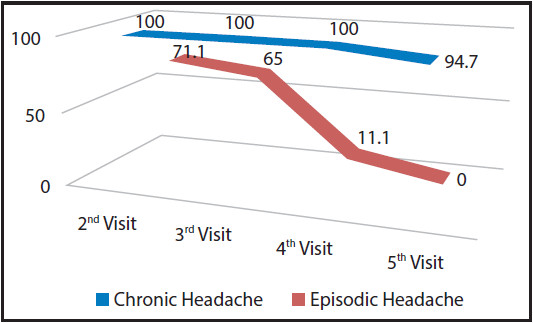
Figure 3: Patient adherence in episodic and chronic headache
In patients with chronic headache, almost 100% of patients showed good compliance and adherence to the treatment resulting in a statistically significant reduction in pain score and headache frequency per week. Further- more, we also found that these patients had received several headache treatments from other hospitals or clinics with unsatisfactory results due to: inadequate patient education about disease progression, the treatment plan, and the side effects of medication.
A challenge for the headache registry program was patient tracking for MIDAS evaluation at the 5th visit. This was because some patients changed their appointment and the alert for MIDAS evaluation disappeared from the computer system. In order to solve this problem, the nurse coordinator will monitor each patient on the appointment schedule to see who still needs to be assessed with the MIDAS questionnaire and make a note in the computer system to notify the team.
The Headache Registry Program provides patient education and encourages patients to take part in planning their treatment. This approach has resulted in good adherence and compliance to treatment accompanied by a significant reduction in the severity and frequency of headache.









