Electronic ISSN 2287-0237
Cancer is a major illness for adolescents globally. In Thailand, for the2010-2012 period, the rate of cancer diagnosed in adolescents agedbetween 10 and 14 years was 10.2 per 100,000 for males and 9.4 per100,000 for females. Among teenagers aged between 15 and 19 years, theincidence rate was found to be 12 per 100,000 for males and 14.6 per 100,000for females.1 Statistical reports from Ramathibodi Hospital in Thailandshowed that the number of adolescents aged between 10 and 15 years whowere diagnosed with cancer was equal to 30 and 29 in 2015 and 2016,respectively.2,3 This study focused specifically on adolescents aged between10 and 15 years, because adolescents older than 15 are admitted to adulttreatment facilities and are treated by non-pediatric physicians. Therefore,they are likely to receive different treatment protocols, which in turn wouldaffect their symptom experiences and QOL.
Adolescents can be treated with various regimens that are usually usedfor both children and adults. They generally receive more intense, longertreatments, and may encounter adverse outcomes when compared to otherage groups.4 These cancer treatments can cause a major disruption toadolescents’ achievement of developmental tasks. Adolescents with cancercannot perform usual activities and tend to depend on their parents, may dropout of school, and this can eventually impact their relationship with friends.This disruption to major developmental milestones leads to poor QOL.5-8Health-related QOL is described as “an overall sense of well-being based onbeing able to participate in usual activities, to interact with others and feelcared about; to cope with uncomfortable physical, emotional and cognitive reactions; and to find meaning in the illness experience”.9 QOLhas been used as an indicator to measure the effectiveness oftreatment during various stages of treatment instead of usingclinical data such as mortality and morbidity.9
Cancer and its treatment can produce multiple symptomsthat affect the QOL of adolescents with cancer duringtreatment.5-8 Adolescents with cancer usually experienceseveral unpleasant symptoms simultaneously, with an averagerange of six to ten symptoms.7-8 Several studies increasinglyfocus on the dimension of multiple symptoms rather than asingle symptom. In particular, the number7, severity5-7, anddistress7-8 of symptoms experienced by adolescents with cancerwere found to be directly related to a lower level of QOL.
Nursing interventions should include an evaluation ofsymptom experiences and its relationship with QOL to managesymptoms effectively and improve better QOL in adolescentswith cancer. Since symptom experiences is an individualsubjective perception there may be variations betweendifferent cultures, leading to different perceptions of QOL.10Children with cancer in Hong Kong who experienced moresevere symptoms reported lower QOL.6 Adolescents withcancer in the United States also perceived lower QOL whenthey were faced with more severe and distressing symptoms.5,7-8In Thailand, several studies have explored multiple symptomsexperienced by younger children but little is known aboutsymptom experiences in adolescents with cancer.11-12 Theperception of symptoms of adolescents maybe differ fromyounger children. Only one study described multiple experiencedsymptoms of adolescents with cancer in terms of severity.11 Itshowed that symptom severity had a negative correlation tofunctional status, which mainly focused on the physical aspectof patients.11 The data about symptom experiences as well asQOL, which shows overall well-being in this unique groupneeds to be explored further in order to improve symptommanagement and QOL. Thus, this study aims to investigatethe relationship between symptom experiences and QOLamong adolescents with cancer receiving cancer treatments inThailand. Consequently, the results will assist in detectingadolescents with cancer who might have poorer QOL and canguide nurses to plan nursing interventions to improve theirQOL.
The Theory of Unpleasant Symptoms (TOUS) developedby Lenz et al.13 was selected as the conceptual framework forthis study. TOUS proposes that symptoms are “perceivedindicators of change in normal functioning as experienced bypatients”. 14 Each symptom consists of four dimensions includingintensity, time, distress, and quality which is influenced bymany influential factors. Generally, several symptoms aresimultaneously perceived by a person. Symptom experiences,therefore can be explained as experiencing multiple symptomsat the same time. The outcome of symptom experiences isperformance including functional and cognitive activities.14Based on this theory, QOL was conceptualized as performancebecause of its domains: physical, emotional, cognitive, andsocial functioning that reflect both types of performance.
This study focused on some particular dimensions of thesymptoms, which were selected based on the literature review.The frequency of symptoms was not included in this study,because it is clear from the study of Collins and associates thatfrequent symptoms are usually reported similarly to severesymptoms.15 In the study framework, symptom experiences(the number of symptoms, symptom severity, and symptomdistress) affects performance and overall QOL in adolescentswith cancer.
This descriptive correlational study consisted ofadolescents with cancer at both the inpatient and outpatientdepartments of Ramathibodi Hospital from February to June2018. This study was approved by the Committee on HumanRights Related to Research Involving Human Subjects,Faculty of Medicine Ramathibodi Hospital, Mahidol University.
The inclusion criteria were as follows:
The calculation for the sample size at the level of power= 80%, α = 0.05; effect size = 0.5 (r = -0.52, the lowestcorrelation coefficient of Baggott and associates7) determinedthat 25 participants were required for this study.
Instruments
Data Analysis
The demographic data, clinical data, symptom experiences,and QOL of participants were analyzed using various conceptsof descriptive statistics. The relationships between each variableof symptom experiences and overall QOL were analyzed usingPearson’s product-moment correlational statistics.
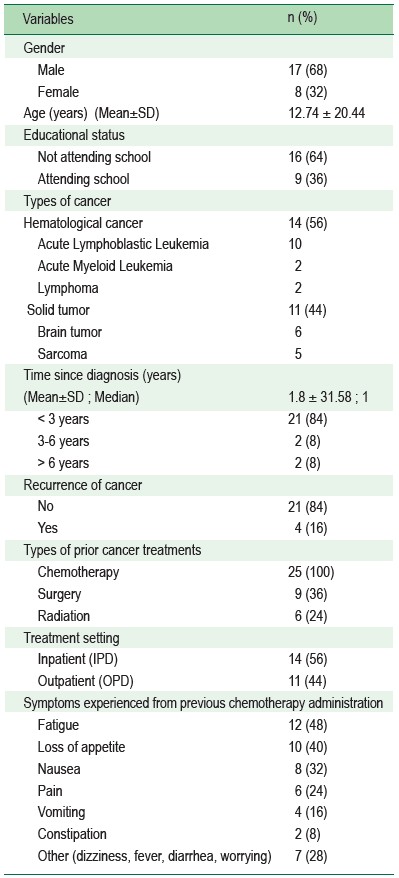
A total of 26 adolescents with cancer met the inclusioncriteria. Only one adolescent declined to participate in thestudy, citing inconvenience as a reason. Therefore, the studysample consisted of 25 adolescents with cancer. The majorityof the adolescents were male (68%) with a mean age of12.74 ± 20.44 years (range = 10.2-15.8 years). Sixteenparticipants (64%) had stopped attending school. The mostcommon cancer diagnoses were hematological cancers (56 %);leukemia (85.7%) and lymphoma (14.3%). The participants’length of time since diagnosis to their entry into the studyranged from 1 to 11 years (1.8 ± 31.58) with most (84%) lessthan 3 years. Thirty-six percent (36%) of the adolescents hadbeen treated with surgery, in addition to chemotherapy, andslightly more than half of them (56%) had been treated asinpatients (Table 1).
Table 1: Demographics and characteristics (n = 25)
Symptom Experiences
According to MSAS 10-18, the participants experienceda mean number of 11.80 ± 5.61 symptoms. The mean ratingof the symptom frequency was 0.82 ± 0.46, with a symptomseverity rate of 0.62 ± 0.41, and a symptom distress rate of0.40 ± 0.42 (Table 2). The number of experienced symptoms,or the prevalence rate of symptoms among the participants,ranged from 1 to 23 symptoms. More than half of the participantsexperienced dry mouth (80%), lack of appetite (68%), and lackof energy (64%) (Table 3). The most frequent symptom was dry mouth (45%), followed by numbness (40%), and lack ofenergy (37.5%). The most severe symptom was swelling ofarms or legs (33.3%) as well as hair loss (30%), and nausea(28.6%). The most distressing symptom was changes in theway food tastes (42.9%) followed by swelling of arms or legs(33.3%), and lack of energy (31.3%). There were differencesin every dimension of each symptom. The prevalence of eachsymptom was not related to its rate of frequency, severity, ordistress. Dry mouth was reported to be the most common andfrequent symptom, but not as the most severe or distressingsymptom for them (Table 4 and Figure 1).
Table 2: The symptom experiences on MSAS 10-18 scores (n = 25)
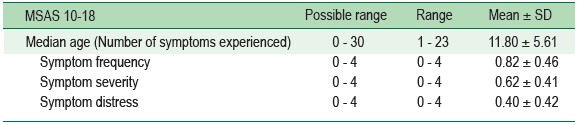
Table 3: The experienced symptoms (n = 25)
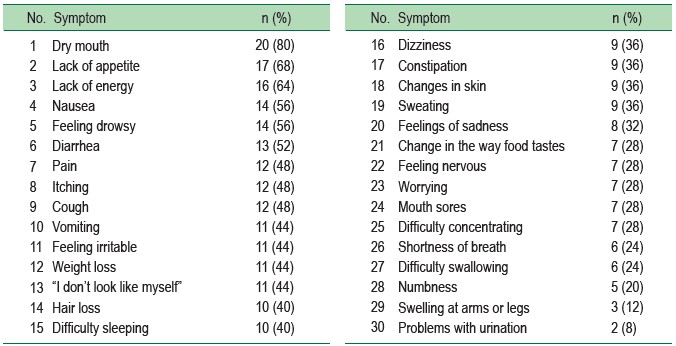
Table 4: The overview of total 30 experienced symptoms by sample in every dimension (n = 25)
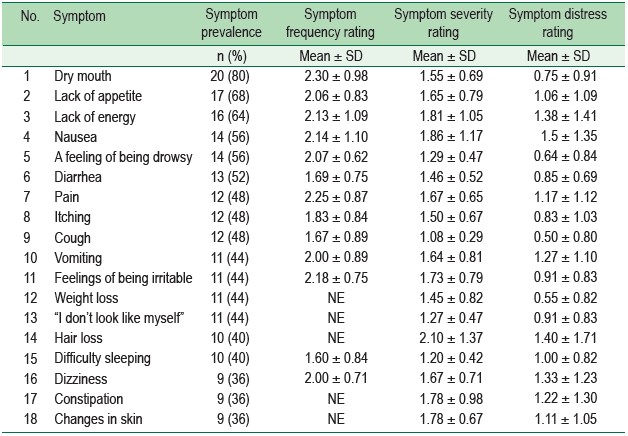
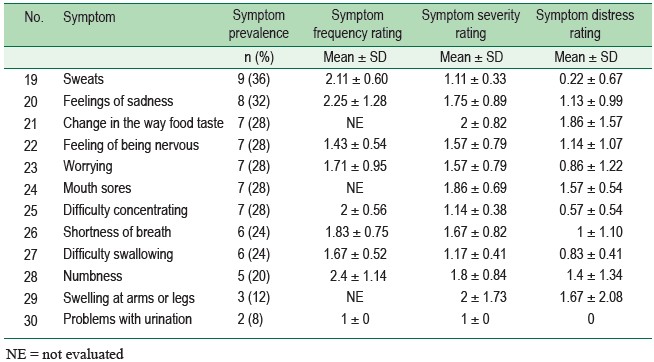
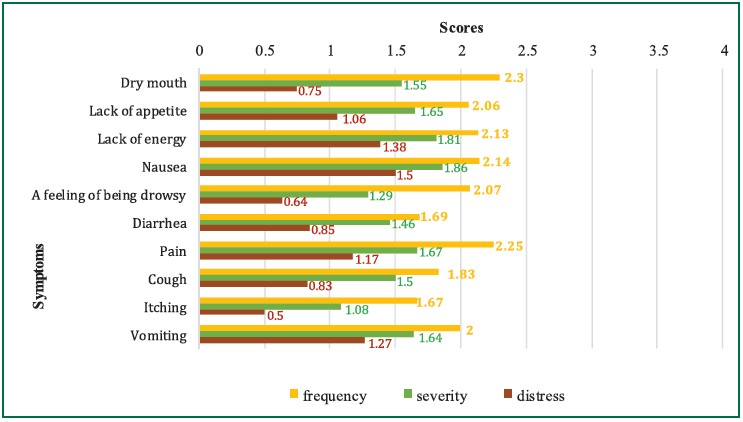
Figure 1: The 10 most prevalent symptoms with mean frequency, severity, and distress ratings
Quality of Life (QOL)
Regarding QOL, the participants reported a mean totalscore of QOL of 72.09 (SD = 16.70). The mean scores of eachaspect of QOL revealed that most of the participants had highscores in the following aspects of their QOL: 1) Social (84scores); 2) Emotional (77.40 scores); 3) School (68.4 scores);and 4) Physical functioning (63.63 scores).
Relationship between Symptom Experiences and QOL
In regards to the correlation between symptom experiencesand QOL, each dimension of symptom experiences (the numberof symptoms experienced; symptom severity; and symptomdistress) was negatively correlated with overall QOL, with thestatistical significance at p < 0.05 (r = -0.597, -0.594, and-0.582).
The result of this study showing that the participantsexperienced a mean of 11.8 symptoms is similar to the studyof Baggott and associates7 (10.6 symptoms). The most prevalentsymptom experienced by the participants was dry mouth. Mostof the participants were in their first year after their diagnosisof cancer, during which patients usually receive intense and frequent treatment cycles. Almost half of them were receivinghigh doses of methotrexate at the time of data collection, andso they mostly experienced dry mouth. Methotrexate generallyaffects normal cells in the same way as malignant cells, andso the healthy cells, especially the oral mucosa, tend to bedamaged. As a result, most patients first experience oral painor dry mouth, followed by oral mucositis.18
Given these reasons, dry mouth was also reported as themost frequent symptom during the first 7 days afterchemotherapy administration. In contrast, Collins and associates15found that problems with urination was the most frequentsymptom in adolescents who were receiving chemotherapyand those who were off treatment, while this study consistedonly of adolescents who were receiving treatment. Therefore,the symptoms were differently perceived by both groups.
In terms of symptom severity, the mean rating of symptomseverity was 0.62 which was similar to Baggott and associates7;0.7. Swelling of the arms or legs was reported as the mostsevere symptom. Most of the chemotherapy agents which theparticipants received were administered intravenously, whichinvolves receiving a large volume of fluid. Most of them werealso given hydration, prior to the administration of theirchemotherapy. Therefore, many of the participants experiencedswelling at arms and/or their legs. Furthermore, inactivityduring hospitalization is another possible reason for experiencingswelling.
In regard to symptom distress, the mean rating was 0.40.Changes in the way food tastes was rated as the most distressingsymptom. Besides methotrexate, vincristine and cyclophosphamidewere given most often to participants. Vincristinedamages several cranial nerves and can lead to changes in aperson’s swallowing and tongue movements, usually leadingto altered taste sensations. Cyclophosphamide also interfereswith the glossopharyngeal nerve, leading to altered perceptionsof taste among patients.19 Patients, consequently, are not ableto eat or drink as usual. In addition, most Thai culinary dishesinvolve a taste combination of sweet, sour, and salt. Therefore,experiencing taste alterations while receiving cancer treatmentcould contribute to loss of appetite, weight loss, and malnutritionwhich can affect the effectiveness of cancer treatments. Thisis why participants perceived changes in food taste as theirmost distressing symptom
Quality of Life (QOL)
According to the results, the participants reported anaverage overall QOL score of 72.09, indicating a high QOL.This was similar to the study done on children in Thailandwith chronic health conditions; 72.7.17 In terms of the subscales,they had a high average QOL, according to social, emotional,school, and physical functioning.
Social functioning was rated with the highest average score(84), showing that these participants had the ability to get alongwith others and to keep contact with their friends. Most ofthem had to stop attending school during their treatments.However, due to the modern technologies of various forms ofsocial networking, the adolescents tended to have the opportunityto keep in contact with their relatives and friends. Therefore,they did not feel different from their healthy friends in termsof social interaction, as shown by their high scores of QOL inthe area of social functioning. In the same way, there was nodifference in this regard for both patients and healthy groups.7,17
The participants reported emotional functioning with anaverage score of 77.4. This can be explained by some aspectsof Thai culture. That is, Thai parents usually encourage theirchildren, using both words and various activities, so that theseparticipants are able to cope with the unpleasant experiencesof both the progression of their disease and the side effects oftheir cancer treatments. Consequently, most of them felt thatthey had not been abandoned to fight cancer alone.20
Adversely, these participants had a low QOL in schoolfunctioning, with an average score of 68.4. Most of them hadstopped attending school during their treatment, causing themto fall behind academically. There was a significant differencebetween the QOL in this area among healthy Thai children andthose with chronic health conditions.17 Likewise, Sandebergand colleagues21 found that those children who did not attendschool while receiving cancer treatment reported a low QOL.The physical functioning obtained the lowest scores amongthese participants, with a mean score of 63.63. This is consistentwith the results of Baggott and team.7
Experiencing symptoms simultaneously forced theparticipants to confront unpleasant physical problems.Consequently, they were not able to perform many activitiesof daily life, thereby leading to a lower QOL. Also, Thai childrenwith chronic health conditions generally had lower scores inthe area of physical functioning than healthy children.17
Relationship between Symptom Experiences and QOL
This study shows that the symptom experiences of adolescentswith cancer (the number of symptoms experienced, symptomseverity, and symptom distress) negatively correlate with theiroverall QOL. This was congruent with the findings of previousstudies.5,7
The number of experienced symptoms had a significantnegative correlation with overall QOL. Experiencing severalsymptoms simultaneously can result in patients being unableto perform daily activities, leading to a low QOL in all areas.In a study conducted by Baggott and associates,7 adolescentswith cancer, while they were receiving treatments, experiencedmore symptoms and reported a lower total QOL, as comparedto those who had fewer symptoms.
Severity of symptoms negatively correlated with QOL, ata significant level of 0.05. The intensity of symptoms perceivedby adolescents with cancer is likely to increase when theyexperience multiple symptoms at the same time with theaccompanying impact on their QOL. This finding was congruentwith several previous studies.5,7
Symptom distress was also found to have a significantnegative correlation with QOL. This is, because, during theircancer treatment regimens, adolescents with cancer generallyexperience various symptoms concurrently, and these cooccurringsymptoms catalyze each other and, thus, tend tocontribute to a low QOL. Similarly, in the study done by Baggottand associates7, most adolescents with cancer also reportedthat distressing symptoms affected their levels of QOL.Moreover, Hinds and associates also discovered that the degreeof symptom distress could predict the QOL among childrenand adolescents who had either acute myeloid leukemia orosteosarcoma.8
Symptom experiences and QOL in adolescents with cancerafter receiving at least one cycle of chemotherapy showsspecific differences in every dimension of each symptom.Therefore nurses are advised to assess every dimension of eachsymptom during chemotherapy for both inpatients andoutpatients to ensure better QOL.
The authors would like to thank all of the participants, whowere the most important part of this successful study. Also,they would like to express their deepest appreciation to all ofthe staff at the pediatric oncology clinics of RamathibodiHospital for their cooperation in the data collection.









