Electronic ISSN 2287-0237
In Thailand, there was a total population of approximately 66.4 million at the end of 2018,1 with an increase of total death from 456,391 to 473,541 cases (from 2015 to 2018).2 The five major causes of death in Thailand are aging, heart failure, sepsis, primary hypertension, and diabetes mellitus.3 The place of death occurs mainly at hospitals and homes. Thus, health care providers, especially nurses, have an opportunity to prepare to care for people who are confronted with death and dying.4,5
Death is a natural phenomena that everyone has to experience and there is no escape from this.5,6 According to the Thai cultural context, death has been perceived as taboo by Thai people. Consequently, they do not talk about death and there is a lack of preparation for death.6 Those nearing death may also face emotional turmoil, including fear of death.4 It causes people to fight for prolonging life, increasingly dependent on medical care services including medicinal use, invasive medical instruments, and cardiopulmonary resuscitation.7 Although these treatments can extend life, these treatments can cause patients physiological, psychosocial, and spiritual suffering.4,6,8
A good death is an important goal of caring for patients with end of life conditions or receiving palliative care.4-10 A good death has not beenuniversally defined because of the differences in individual perception, belief, and sociocultural context. Moreover, the meaning of a good death is different depending on patient’s views, families, and health care providers. This may affect the patients’ care in promoting a good death.4-6, 8-11
Thailand is different from western countries, particularly when it comes to spiritual and religious beliefs that are integral to the Thai way of life from the beginning of life to the end of life. The majority of Thai people are Buddhist accounting for more than 90%, Muslims accounting for 4% of the population, and others.9,11,13 The difference in sociocultural context and belief have influenced the perception of good death among patients, families, and health care providers, which may be different in their views. Nurses have played important roles to promote a good death for patients nearing death.4-6 Deep understanding of a good death from a nurse’s perception is crucial for providing care to promote a peaceful death.
However, previous studies on the perception of Thai nurses on what constitutes a good death are based on limited knowledge since there were only four authors and eight studies on this subject. Furthermore, most of the studies are single research studies in different areas and samples. For instance, four studies explored and described the concept of a peaceful death and the care experience for persons with peaceful death among Buddhist ICU nurses in Southern Thailand,10-13 whereas only one study described peaceful death among Muslim nurses in Southern Thailand.8 Besides this, two studies described good death nursing care among Buddhist nurses in Eastern Thailand.4-5 In addition, one study explored Buddhist nurse’s experiences of a good death in Southeastern Thailand.5 The research results from these studies were similar and different in the meaning of good death and the care experiences among Thai nurses. Therefore, this review will be expected to fill the gap or indicate the existing knowledge and need further research. An integrative review of good death on Thai nurses’ perception can provide the deep understanding of good death that is beneficial for developing nursing theory, nursing practice and policy suggestion to promote good death for the end of life patients.14
This integrative review based on Whittemore & Knaft’s method with five stages as follows.14
1. Problem identification stage; this stage is to clearly identify the problem. An appropriate-specified research problem will facilitate to define accurately operationalize variables or sampling frame. The purpose of this study was to review the meaning of good death and the care experiences of Thai nurses’ perceptions. Thus, the question of this review was identified as ‘what is the meaning of a good death and Thai nurses’ perceptions of care experiences?’
2. Literature search stage; this stage is to search the literature reviews from various methods including hand-searching and networking to reduce bias. This process should be clearly documented including the search term, the databases used, additional search strategies, and the inclusion and exclusion criteria for determining relevant primary sources. Thus, the keywords, both Thai and English words, were used for searching in this integrative review including; “good death”, “perception” “experience”, “nurse”, “Thailand”, “patient”. ThaiLIS, ThaiJO, PubMed, CINAHL, ProQuest, and ScienceDirect were used for research searching from January 1st, 2009 to March 31st, 2019. Inclusion criteria consisted of
1) Qualitative study
2) Studying of Thai nurses’ perception of a good death Thai nurses’ perception
3) Studying in Thailand
4) Primary source.
3. Data evaluation stage; this stage is to evaluate the quality of primary sources including empirical and theoretical reports. In a review that encompasses theoretical and empirical sources, it requires two quality instruments to use as the inclusion and exclusion criteria or as a variable to identify the concept of integration. The Critical Appraisal Skills Programme (CASP) with ten items was used to evaluate the quality of qualitative studies.15 Three characteristics of answer included yes, cannot tell, and no. Research studies were included in the study that meet at least 6 items or 60 % of the data evaluation criteria fromtwo reviewers. The steps of data evaluation is presented at Figure 1.
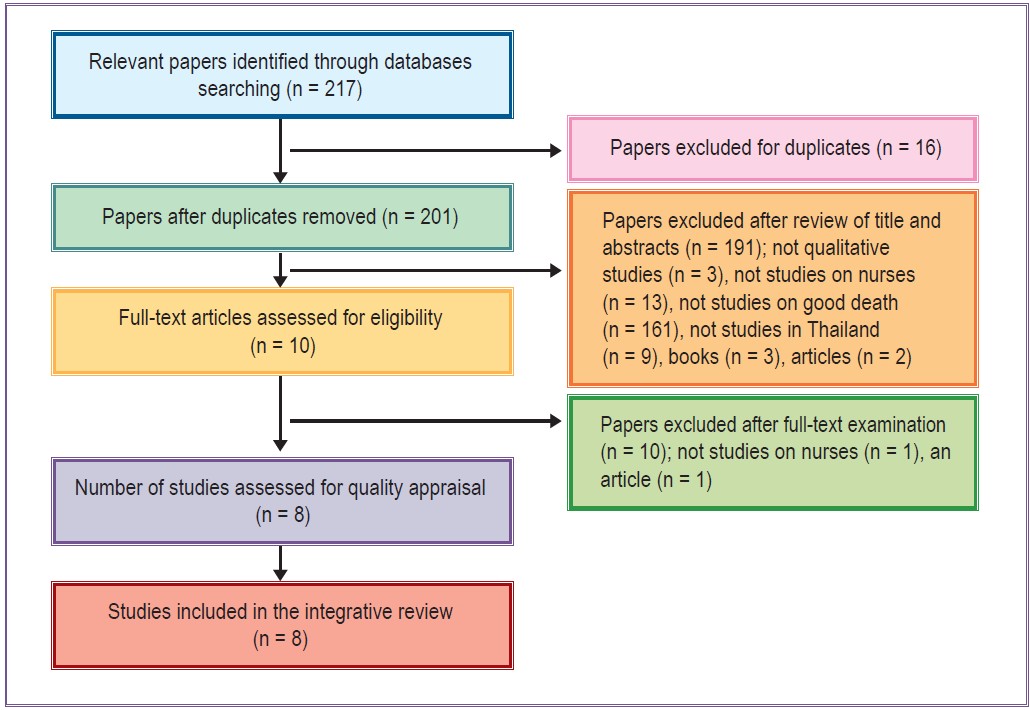
Figure 1: Flow chart of search results
4. Data analysis stage; this stage is to order, code, categorize, and summarize the data from primary sources into a unified and integrated conclusion. Whittemore & Knaft14 suggested that data analysis includes;
1) Data reduction is used to divide the primary sources into subgroups depending on the type of research design, chronological, setting, sample characteristics, and a predetermined conceptual classification. Then, extracting and coding data from primary sources into a matrix or spreadsheet to compare primary sources on specific issues, variables, or sample characteristics.
2) Data display involves converting the data extraction from primary sources into a display in the form of matrices, graphs, charts, or networks and set the stage for comparison across primary sources. The display illustrates the patterns and relationship of the primary data sources and serves as an initial point for interpretation.
3) Data comparison is the stage to identify patterns, themes, or relationships. It can prepare clarity to the empirical and theoretical support emerging from early interpretation.
4) Conclusion drawing and verification is the final phase of data analysis. The primary sources were reviewed to verify the new conceptualization at higher levels of abstraction that was consistent with primary sources. In the integrative review, we extracted and coded data from eight studies by using the summarized table to reduce data, compare data, and conclude data into new themes in order to present the results from the review about Thai nurses’ views of a good death (see Table 2 and 3)
5. Presentation: This stage aims to present the results of the study. It can be applied for nursing practice, creating a nursing theory, and policy suggestion to promote good death for the end of life patients.
Table 1 : Selecting articles that were relevant
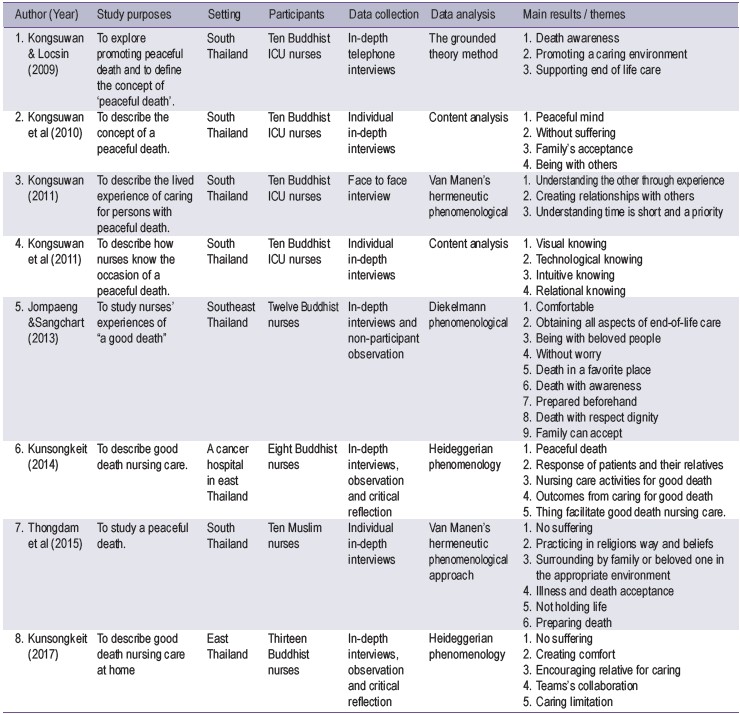
Table 2 : Themes of integrative reviews
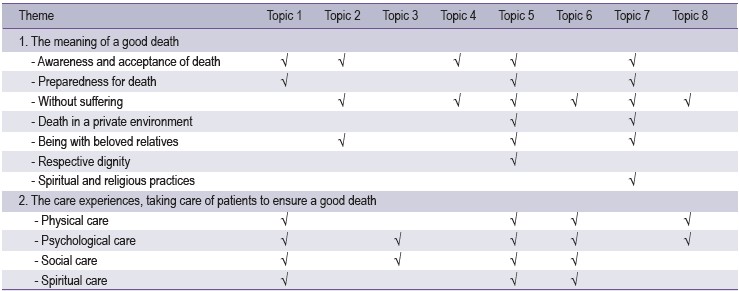
The results revealed that there were two themes of integrative review: 1) The meaning of a good death, and 2) The care experiences of Thai nurses to take care of patients to ensure a good death.
1. The meaning of a good death. Thai nurses’ perception of the meaning of a good death included awareness and acceptance of death, preparedness for death, without suffering, death in a private environment, being with beloved relatives, respecting dignity, and spiritual and religious practices. The details are described as follows.
Awareness and acceptance of death Participants perceived that awareness and acceptance of death could promote a good death.6,10,11 They perceived that death was a natural event. Everyone has to experience birth, sickness, old age, and death. Nobody can escape from this situation. Therefore, they are always concerned about death and being careful in their daily lives. In addition, while they had to confront death, they had a conscious and peaceful death.6,8-10 As an example, in the word of participants:
“Peaceful death is ...both family members and patients accept their status and end of life date. They want to pass away with a peaceful mind”8
Preparedness for death: Participants perceived that preparing for death is important for promoting a good death, which was the need for responses, selecting the death place, making merits, and saying goodbye to family members.6,8,11 As an example, in the word of participants:
“Cases with good preparing...They communicate with their family. For example, which is the favorite place for death hospital or home. These cases have prepared the place for their good death”6
Without suffering : Participants perceived that the absence of suffering, either physical or psychological, could promote a peaceful death. Without suffering meant that patients were physically comfortable, in no pain, no longer suffering from disease symptoms, with no invasive medical instruments, no cardiopulmonary resuscitation or electrical cardioversion and defibrillation to prolong their life, a death without worry.4-6,8 As an example, in the word of participants:
“There pass away no suffering. Breathing is slow, not suffering, and without medical instruments called good death”5
Death in a private environment : Participants perceived that death in a private place at the hospital or home, where the atmosphere is familiar with quiet surroundings with their relatives and without crying, could promote good death.4,6,8 As an example, in the word of participants:
“I think quiet environment leads patients being peaceful mind and they can be with their relative leading them to die with peace”6
Being with beloved relatives: Participants perceived that being with beloved relatives could help to promote a good death. Participants do not feel alone, warm, secured, and without the fear of death. Moreover, they had the opportunity to feel the love and care from their relative, say goodbye, and forgive on the last breath. These were crucial for supporting a good death.6,8,10 As an example, in the word of participants:
“I think sometimes patient want to meet their relatives who never meet or don’t visit them [‘ma-du-jai,’ in the Thai language], they may have something to talk and say goodbye”4
Respecting dignity : Participants perceived that respecting dignity was very important for promoting a good death. Although patients have passed away, nurses still should still be concerned and respect their dignity.6,11 As an example, in the word of participants:
“Muslim felt when they are admitted to the hospital, that their dignity is gone in the second they walk into the hospital. Their humanness is thrown away because they are taking off their clothes and have no privacy. It is like their humanness is ruined”11
Spiritual and religious practices: Participants perceived that spiritual and religious practices are crucial for supporting a good death. Buddhist Thai nurses believed that inviting a monk to pray for patients, reading dharma book, or listening to dharma from CDs could promote a good death.4,5 Muslim Thai Nurses believed that reading Ya-seen or Al-Quran could remind patients to pay attention to God and also promote a good death.8,11 As an example, in the word of participants:
“We believed, if they think of the good things, they will get the peaceful mind, happiness, and they’re going to a good place after death. According to religious laws, Buddhist who listen to the dharma from CDs or praying may have mind anchor to bring for the good thing”5
“Reading Qur’an near the patients and patients pray, if patient unconscious, a family member will pray for them so that they close to Allah ....”8
2. Care experiences of Thai nurses to take care of patients to ensure a good death.
The care experiences of Thai nurses to take care of patients to ensure a good death included physical, psychological, social, and spiritual care that required holistic care from nurses. The details are described as follows.
Physical care: Participants indicated that physical care was an important key to promote a good death for patients including promoting physical comfort, alleviating pain and managing the symptom of diseases.4-6,11 As an example, in the word of participants:
“We do not take it (treatment) for granted. We feed them, elimination care, bathing, giving pain killer and comfort”4
Psychological care: Participants indicated that psychological care was a crucial care to promote a good death for patients consisting of eliminating fear, anxiety, and loneliness by responding to patients and to their families’ needs, giving information, touching, and emotional support.4-6,11 As an example, in the word of participants:
“Nurses should care by heart...doing everything by heart for patients and their families. They can perceive that we serve them. They will trust and accept our suggestion. They feel warm and passed away with a good death”5
Social care : Participants indicated that social care was a vital role to promote a good death for patients including allowing the opportunity for family members to take care of their relatives at the end of life.4,6,11,12 Preparing care for family members by assessing family’s readiness, giving advice, and participating in care was important to promote a good death.4-6 As an example, in the word of participants:
“Family members are important for patients if they have a chance to take care of patients. The patients will be warm... We should allow family members to take care of them”5
Spiritual care: Participants indicated that spiritual care is important to promote a good death for patients including spiritual and religious practices by creating a calm environment for praying or doing meditation, inviting religious leaders to pray or talk with patients, and serving Dharma book orBible.4,6,11
As an example, in the word of participants:
“We advise patients to use Dharma for assisting them to be conscious and attentive. We ask them first and give them for listening to Dharma every day. They can calm and sleep well”4
According to the review, there were two themes of the integrative review: 1) The meaning of a good death, and 2) The care experiences of Thai nurses to take care of patients to ensure a good death. This is explained according to each theme as follow:
1. The meaning of a good death. Awareness and acceptance of death:
Participants perceived that awareness and acceptance of death could promote a good death. Buddhist teachings and beliefs are integral to the Thai way of life, from birth to the end of life. Buddhists believe that everybody has to experience the natural law consisting of birth, sickness, old age, and death, which is called ‘Samsara’6. Awareness of Samsara law can remind Thai Buddhists to be aware of and to accept death. Moreover, they are often concerned that time is short and is a priority. Thus, while they are still alive, they try to do good deeds, such as making merit, in order to remember them before they die. As a result, they can have a conscious and peaceful death.10 Similarly, Thai Muslims also believed that humans cannot escape from birth, sickness, old age, and death. Illness and death is God’s will. Allah gives life for all human and they have to come back to him.8 While most people in western countries are Christian. They believe that illness is God’s will and death is rebirth in heaven, prepared by God.10
Preparedness for death : Participants perceived that preparing for death is vital to encourage a good death. Preparedness for death includes responding to patients’ needs, saying words of forgiveness and saying goodbye, selecting the place of death, making merits, and performing the funeral rites.6,8,11 These activities can assist patients to prepare their mind, respond to their needs, eliminate worries, accept death, and confront death with a peaceful mind and consciousness.6,8
Without suffering : Participants perceived that a good death was a death without physiological and psychological suffering, no invasive medical instruments and no worries about death.4-6,8 Thai Buddhists perceive that the most important need for end of life patients is that they can leave from this world with a peaceful mind without suffering, either physiological or psychological, and they also don’t want to prolong their life by invasive medical instruments.8 Thai Muslims perceive that invasive medical instruments or CPR can cause patients spiritual pain. Death is God’s will, which is prepared by him and it will bring patients to God’s hand. Therefore, health care providers and nurses should allow patients to die in peace instead of prolonging their life.10
Death in a private environment : Participants perceived that death in a private place at home or in hospital surrounded by beloved relatives, a familiar environment, a quiet place, and without crying could improve the sense of warmth and security. This supported patients to have a good death.4,6,10 Thaipeople believe that death in a familiar place, a quiet atmosphere, without crying by relatives can assist patients to release worries, increase consciousness, pay attention to the good things. These can bring patients to a good place or heaven after they pass away.6
Being with beloved relatives : Participants perceived that patients being with relatives improved the sense of belonging, not feeling alone, feeling warm, feeling secure. Moreover, patients and their relatives had an opportunity to give and receive forgiveness and to say goodbye one last time and to let them leave with a peaceful mind.4,6,10 The result of this review is congruent with the concept of end of life care and palliative care in Thai Buddhism. The value and meaning for Thai Buddhist patients nearing death is enhanced when they are surrounded by their relatives, having an opportunity tomeet and say goodbye, and not remaining alone. These factors can support patients to have a good death. It is also congruent with the Muslims’ beliefs. They believe that staying with relatives for forgiveness (Ma-Af), and saying goodbye is important for promoting a good death.10
Respecting dignity : Participants perceived that respecting patients’ dignity was important for promoting a good death. Nurses should respect patients, both still alive and those who have passed away.6,11 Thai Muslims believe that the body of a patient after death has a sense of pain. Thus, Nurses should respect the dead person’s body. For example, they should ask for permission every time before each nursing practice cleaning the body, and they should not expose the body of dead persons10.
Spiritual and religious practices : Participants perceived that spiritual and religious practices were essential for promoting a good death. Thai Buddhists believe that inviting a monk to pray, reading dharma books, and listening to dharma books from CDs were crucial to bringing patients’ mind to a good place or heaven.4,5 Likewise Thai Muslims believe that reading Ya-Seen or Qur’an for patients reminds them to remember Allah and to promote peaceful death.10,11 Thai Christians believe that end of life patients need to meet the pastor, pray, read the Holy Bible. These help people who believe in God. The soul will be cleaned by God and brought back to heaven which is prepared by God.10
2. The care experiences of Thai nurses to take care of patients to ensure a good death.
The care experiences to take care of patients to ensure a good death was holistic care consisting of physical, psychological, social, and spiritual care. Holistic care is a philosophy of nursing profession where each human is a whole human being consisting of the physical, psychological, social, and spiritual dimensions. Therefore, the goal of all nursing practices is to care for the whole person.6 Physical care is important to alleviate pain, decreasing symptom distress from the diseases and promoting comfort which supports patients to experience a good death. 4-6,11 Moreover, psychological care is important to eliminate emotional troubles of patients and their families during the time of death with a peaceful mind. 4-6,11-12 Furthermore, social care is important to promote a good death for patients by preparing family members’ readiness, family participation and responding to their needs. 4-6,11 In addition, spiritual care is important to encourage a good death for patients by allowing the opportunity for patients and their families to do spiritual and religious practices.4,6,11 Harai et al.16 and Costello17 indicated that a good death required holistic care for patients.
This integrative review provides a deep understanding of Thai nurses’ perceptions of a good death. Seven themes emerged and were synthesized, consisting of the meaning of a good death; awareness and acceptance of death, preparedness for death, without suffering, death in a private environment, being with beloved relatives, respecting dignity, and spiritual and religious practices, and the care experiences of Thai nurses to take care of patients to ensure a good death consisting of physical, psychological, social, and spiritual care. The findings are important to apply to palliative and end of life care to promote a peaceful death.
The findings from this review can be used for developing a concrete nursing guideline to promote a good death for end of life patients. For instance, nursing training programs, assessing and responding to patient and family needs, family participation, and preparedness, patients and their family’s program to face death. An integrative review of the patient’s perception and family’s perception should be explored for further studies.
This integrative review focused on qualitative studies on Thai nurses’ perceptions of a good death. Therefore, the results refer only to the Thai cultural context. This review also focused on nurses’ perceptions. Thus, the meaning of a good death may differ from the viewpoint of patients, their families, and other health care providers. Besides, there were six databases including ThaiLIS, ThaiJO, PubMed, CINAHL, ProQuest, and ScienceDirect for searching data, and some studies were not included in this review. Further studies should explore the meaning of a good death from the perspective of patients, family, and other health care providers with more countries and databases in order to better understand what constitutes a good death. Nursing care for promoting a good death and factors involved to promote a good death should be explored.









