Electronic ISSN 2287-0237
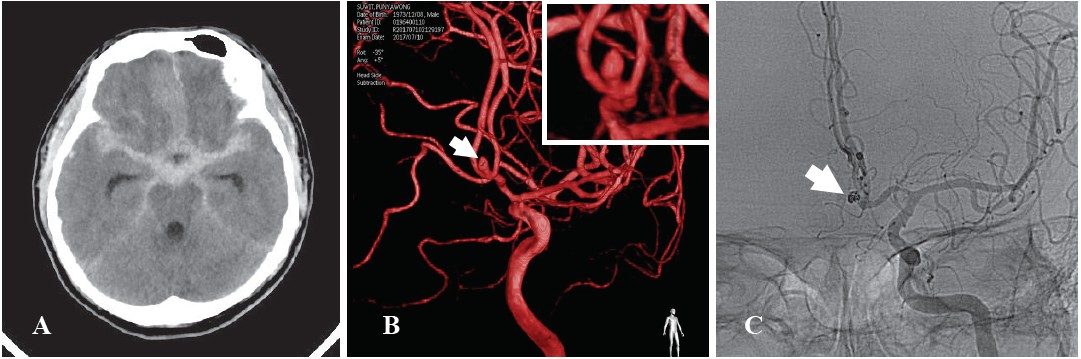
A43-year-old healthy man presents with a sudden severe headache during a weight lifting exercise. No underlyingdiabetes mellitus or hypertension known. He is a moderate alcoholic drinker and smoker. All laboratory findings areunremarkable except mild elevation of high density lipoprotein (HDL); 53 mg/dL), normal range is within 50 mg/dL.Computed tomography (CT) of brain without contrast enhancement reveals diffuse thick acute subarachnoidal hemorrhage alongcisterns. Bilateral fronto-anterior temporal lobes edema is seen. Subfalcine herniation contralaterally shift leftward is remarked(see Figure A). Selective left internal carotid arteriogram reveals 2.4x2.5x3.9 mm saccular aneurysm at anterior communicatingartery (aCom) with a 1.5 mm neck width. Three-dimensional (3D) reconstruction of intracranial artery before coiling is identified(see Figure B arrow). Endovascular coiling was performed with a 6F Softtip guiding catheter inserting to the tip at distal cervicalportion of left intracranial internal carotid artery (ICA). Successful coiling using 2 microcoils (Target, Stryker), measuring2mmx4cm and 1mmx1cm at the aneurismal site was performed (see Figure C arrow). In conjunction with an external ventriculardrain, eventually he fully recovered without any neurological deficit. According to the Radiology Review Manual 7th edition1the rate of cases presenting with aneurysm of aCom at autopsy is 25% and by angiography with symptoms is 36% and the riskof bleeding is 70%. Ayman Z Ahmed et al.2 analyzed 15 cases that underwent both microsurgical clipping and endovascularcoiling. The rate of mortality after clipping is 26.7% and after coiling is 6.7%. According to the Glasgow Outcome Scale (GOS)at the 6 months follow up, Scale 5 is considered a good recovery in clipping (8 cases) and in coiling (9 cases). The recurrencerate of clipping is 0% and the coiling technique is 26.7%.
In conclusion, in a proper clinical setting, when compared to microsurgical clipping, endovascular coiling is preferable inthe management of a ruptured aCom aneurysm as well as being less invasive and with a lower mortality incidence. This case isa sample case demonstrating the successful endovascular coiling of an aCom aneurysm without any neurological deficit.









