Electronic ISSN 2287-0237
Simple rib fractures are the most common injury sustained followingblunt chest trauma, accounting for more than half of the thoracicinjuries that result from nonpenetrating trauma. Approximately 10%of all patients admitted after blunt chest trauma have one or more ribfractures. These fractures are rarely life-threatening but can be an externalmarker of severe visceral injury inside the abdomen and the chest.
First-rib fractures are considered to be an indicator of increased morbidityand mortality in major trauma. According to one study from the UK TraumaAudit and Research Network, a first-rib fracture is a significant predictor ofinjury severity (Injury Severity Score >15) and polytrauma.
Multiple rib fractures are very common in patients with thoracic traumaand are associated with significant morbidity and mortality rates especiallyin patients with flail chest injuries.1 A flail chest injury is defined as at leastthree adjacent ribs fracturing in which there are fractures in at least twoplaces. Flail chest injury presents with paradoxical movement of the chestwall that leads to inadequate breathing and ventilation, pulmonary dysfunction,and potential lung infection.1-3 The reported mortality rate in flail chestinjury is about 10-33%1,2. Multiple rib fractures can lead to respiratoryinsufficiency due to pulmonary contusion, intrathoracic organ injuries, andsevere pain with chest wall movement. Respiratory insufficiency can leadto significant morbidity and mortality rates.2,4,5
Conservative treatment of multiple rib fractures is a standard treatmentthat consists of acute pain management such as analgesic medication andintercostal nerve block,6 a mechanical ventilator and pulmonary hygiene.However, in some patients, conservative treatment may result in a prolongedintensive care units (ICU) stay, pulmonary complications or prolongedintubation.6,10
A recent meta-analysis showed rib fixation for flail chest can reducemortality, lead to a shorter hospital stay, and lower incidences of pneumoniaand the need for a tracheostomy compared to non-operative treatments.7,8However, there was insufficient data supporting rib fixation in cases ofmultiple rib fractures without a flail segment.
In Thailand, rib fixation is a relatively new procedure andthe procedure’s advantages are doubted. However, based onthe evidence that supports the use of rib fixation, especially incases of flail chest injury, the authors of this study developeda guideline for rib fracture fixation aimed to reduce morbidityand mortality in patients who have a flail chest or multiple ribfractures injury (Figure 1). The contraindications of rib fixationare severe pulmonary contusion, severe head injury, and spinalinjury (precluding lateral decubitus position).9
In this study, we aimed to report the outcomes from threepatients who underwent rib fracture fixation. The operationswere performed by four surgeons (two orthopedic traumasurgeons and two cardiovascular surgeons) who attended aThoracic instructional course cadaveric workshop MatrixRIBsystem for sternal and rib fixation. All cases in our series useMatrixRib system (Synthes).
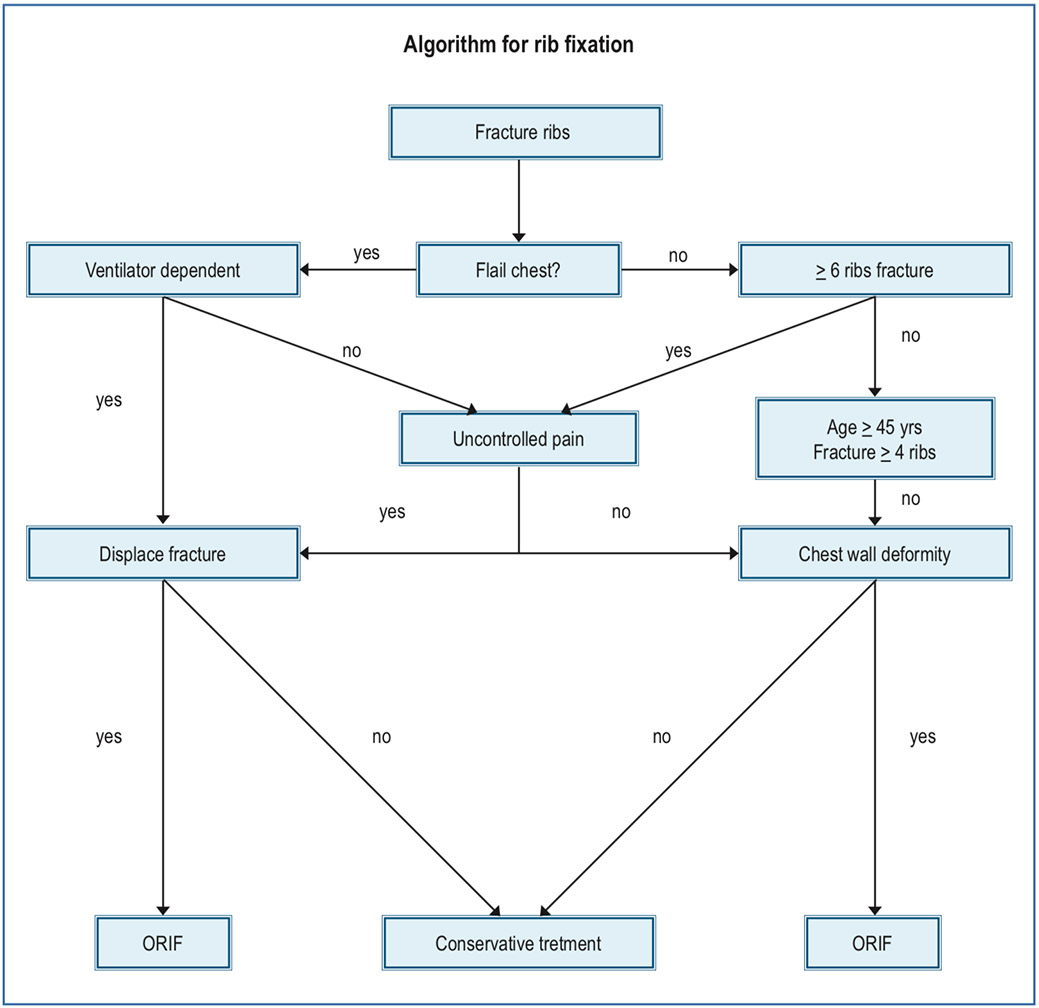
Figure 1: Algorithm for rib fixation at Bangkok Hospital Headquarters (modified from “Rib fractures: To fix or not to fix? An
evidence-based Algorithm” Micheal Bemelmann, et al.
A 55 year old man suffered from traumatic injury resultingfrom a motorcycle accident. Using the Glasgow coma scale,the patient was found to be unconscious with a score ofE1VtM2 .Furthermore, the patient was diagnosed with aparaplegic condition with T11 burst fracture and multiple rightribs fracture with flail chest. In addition, the patient wasdetected pneumothorax and was initially managed and treatedby intercostal drainage (ICD), see Figure 2.
The patient’s injury was re-examined and it was confirmedthat he had sustained a burst fracture with paraplegia resultingfrom spinal cord transecting. The patient was assisted withcontinuous mandatory ventilation (CMV) mode, ICD drainageon the fifth chest. On the 6th day following the injury, the patientunderwent spinal surgery with pedicular screw fixation fromT9 to L1 and decompression. After spinal fixation, the patientused ventilator support pressure controlled ventilation (PCV)mode, PEEP 5 cmH2O, FiO2 0.35. Further diagnosis showedthat he suffered with pneumonia due to obstruction withrespiratory secretions. With the condition of flail chest andbeing ventilator dependent, the team decided to use rib fixationapproach. In general, the contraindication to rib fixationincludes spinal fracture with the exception of this case wherethe spinal cord and nerve roots has been initially fixedappropriately, rib fixation could be performed. At 10th dayafter injury, the ultrasound was used to mark the location atthe 3rd - 6th rib before incision (Figure 2A - B) and the teamoperated rib fixation, anterolateral right rib 3rd - 6th withanterolateral approach (Figure2C).
Skin incision was performed in the oblique fashion atanterolateral chest wall, subcutaneous exposure thensubperiosteal elevated serratus anterior muscle from theirorigin (Figure 2D). Reduction of rib 3rd - 6th was performed bygentle direct reduction and remaining aware to avoid pleuralinjury below the ribs (Figure 2E). Three anatomical plates andone universal plate 8 holes were used and fixed with threelocking screws on each side of the fracture (Figure 2F). Onthe 1st post-operative day, the patient used ventilator PCVmode, PEEP 8, FiO2 0.4, which helped to clear up the secretion.On the 2nd post-operative day, his ventilation improved, andhe was able to use synchronized intermittent mechanicalventilation (SIMV) mode, pressure support 10 PEEP 8, FiO20.5. From the 3rd - 7th post-operative day, he used ventilatorcontinuous positive airway pressure (CPAP) mode, PEEP 8,FiO2 0.3 with oxygen saturation 98-100%. His secretiondecreased, with fewer fever peaks. He was referred back toAustralia on the 9th day after rib fixation with stablehemodynamic, no fever, GCS E3V4M4. Yet, he remainedparaplegic and required ventilator aids in CPAP mode, PEEP10, Fio2 0.3. After rib fixation, it was found that his ventilationhad improved from full ventilator support CMV mode to CPAPmode and lung secretion also improved.
In this case, we decided only to fix the anterolateral fracturesite at each rib due to the posterior site and the skin incisionclose to the surgical wound of the spinal fixation as they maybe future problems from the skin bridge and an increased riskof infection.
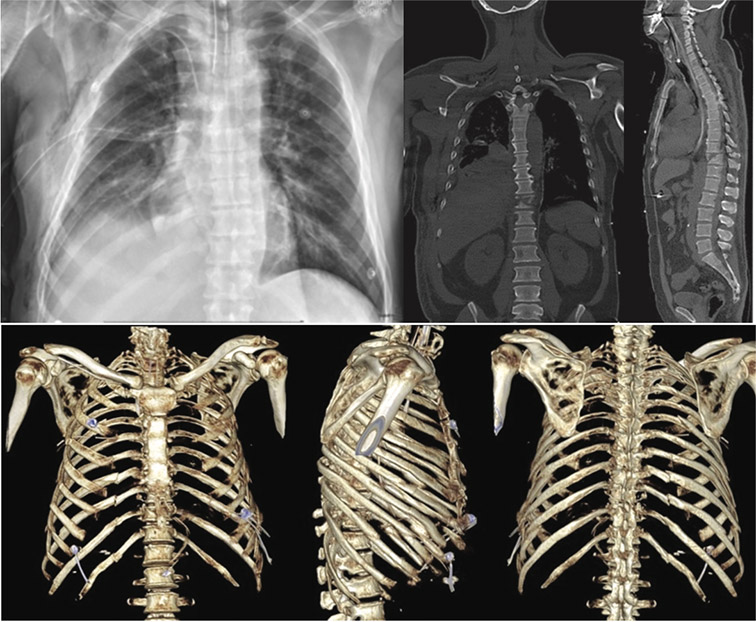
Figure 2: X-ray and computed tomography (CT) scan show multiple right ribs fracture (rib 2nd - 11th) with flail chest.
Figure 2A-B: show lateral decubitus position (2A) and ultrasound landmark for rib 3rd - 6th (2B).
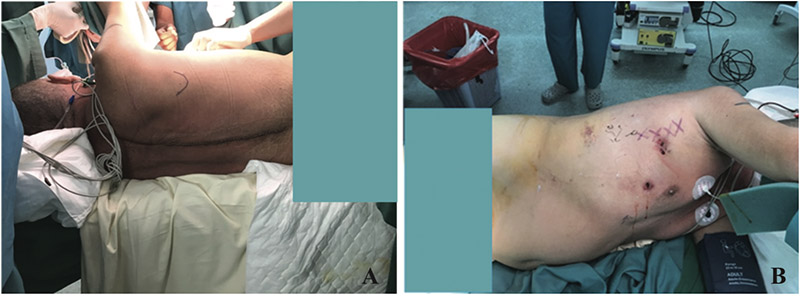
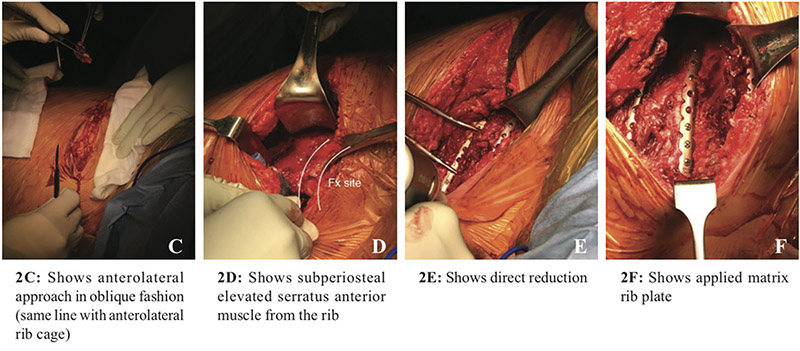
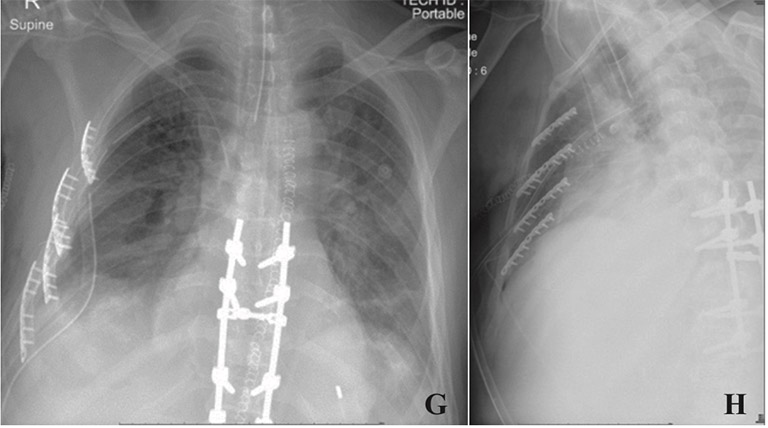
Figure 2G-H: Show post-operation x-rays after fixation 3rd - 6th rib
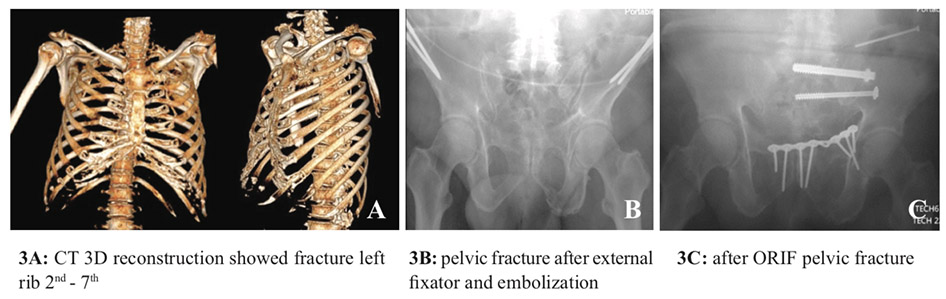
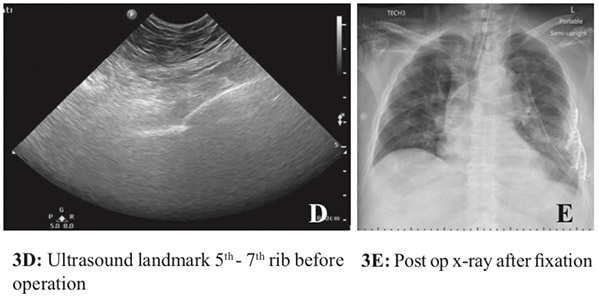
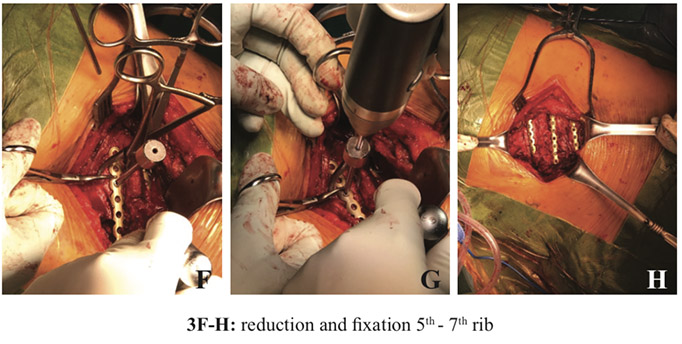
A male aged 82 years old, had a car accident and was sentfirst to another hospital. He had hypovolemic shock (bloodpressure 70/40 mmHg) and remained conscious (GCSE3V1M5) then he was intubated and fluid resuscitation wasadministered. He had cardiac arrest and underwent CPR for15 minutes. He was referred to our center after stabilization,intubated with an endotracheal tube and ICD. From the secondarysurvey, he had head injury, fractures of the left 2nd - 7th ribswith pneumothorax (Figure 3A), pelvic fracture (lateralcompression II) and blood pressure was still borderline. Hewas sent to the operating room for pelvic stabilization with anexternal fixator and embolization superior gluteal artery(Figure 3B). After the surgery, his vital signs were stable andhe was put on the ventilator for full support in CMV mode. Aweek after his surgery, his ventilation had improved, he wasable to use CPAP mode and he then underwent ORIF pelvicfracture (Figure 3C). Then, 3 days after definite fixation ofpelvic fracture, the endotracheal tube was extubated. Due topain during breathing of left chest wall and inadequate breathing,4 days after he had been extubated he was re-intubated withthe endotracheal tube again with pressure support mode. Theteam decided to perform ORIF to his left rib due to beingventilator dependent and in uncontrolled pain with displacedfracture of ribs (2 weeks after his injury). Operative planningof fixation of left 5th - 7th ribs used ultrasound to locate skinincision before operation (Figure 3D). With an anterolateralapproach, and subperiosteal elevation of serratus anteriormuscle then exposed to fracture site, reduction was done bydirect reduction, three universal plate 8 holes were used andfixed with three locking screws on each side of the fracture(Figure 3E - H).
After rib fixation, on the 1st post-operative day, the patientwas weaned off the ventilator with T-piece, FiO2 0.4 and onthe 5th day after rib fixation he was extubated and hadspontaneous breathing with O2 support. On the 6th day afterthe operation he was transferred back to Germany with O2cannula support.
A male aged 74 years old, had a car accident and was sentto a nearby local hospital. Once he was stabilized, he was thenreferred to our center. It was diagnosed with left 2nd - 7th ribsfracture with flail chest and multiple right 2nd - 7th ribs fractureswith bilateral hemopneumothorax. The team initially treatedICD on both sides, fracture sternum, moderate head injury(E3VTM6), closed fracture isolated left tibia, closed fractureright clavicle (Figure 4). At first, he sustained ventilator supportwith CMV mode, PEEP 5 cmH2O, FiO2 0.65 on admission.He had severe pain on both sides of the chest wall, and on the3rd day after injury he underwent intercostal steroid injectionfor controlled pain. Although his clinical condition improvedhe was still unable to move or ambulate properly from the beddue to chest wall pain both sides. On the 7th day of admission,he used ventilator in pressure support 12 cmH2O, CPAP 10cmH2O, FiO2 0.3 but still had pain at both chest walls. He wasoperated and toilet bronchoscopy was applied, with chest washout due to clot of hemothorax and secretion obstruction. Asmall amount of blood clot was found, and a mucous plug inright lower lung. On the 9th day, he was still using the ventilatorin pressure support mode and still had pain on both chest wallsand moderate lung secretion. On the 10th day he underwent ribfracture fixation for both sides due to marked displacement ofribs fracture and uncontrolled pain. The team operated withleft decubitus position to fixed anterolateral site of right 3rd-5thribs first with anterolateral approach. The 4th rib was directlyreduced and fixed with 8 - holes anatomical plate.Subsequently, the 3rd rib was exposed. As the fracture locationof the 3rd rib underneath the scapula was inaccessible for plateand screw fixation, the authors stabilized the 3rd rib by usingVicryl 2-0 tied to the 4th rib as a buddy splint stabilization(Figure 4A). Then the right 5th rib was reduced and fixed with8-holes anatomical plate and 3 locking screws on each side ofthe fracture (Figure 4B). Afterwards, the patient was turned toright lateral decubitus to fix left 4th - 7th ribs through anterolateralapproach. Due to segmental fracture, a 17 - holes anatomicalplate was fixed to left 6th - 7th ribs with 10 and 8 locking screwsrespectively. Then 4th - 5th ribs were reduced and fixed withuniversal plate with 3 locking screws on each side of thefracture (Figure 4C).
On the 2nd post-operative day, the patient was on a ventilatorin pressure support mode, 8 cmH2O, PEEP 5 cmH2O, FiO2 0.3.On the 3rd post-operative day, he was weaned off the ventilatorwith T-piece FiO2 0.3 and extubated on the 4th day after theoperation. He developed acute cholecystitis during admissionand underwent percutaneous cholecystostomy drainage, hisclinical condition improved subsequently. After he wasclinically stable, without fever, we operated with a plate andscrews on his left tibia (Figure 4E). For the clavicle fracturewe treated this conservatively with an arm sling. He wastransferred to the ward to continue rehabilitation. He wasdischarged 3 months after injury.
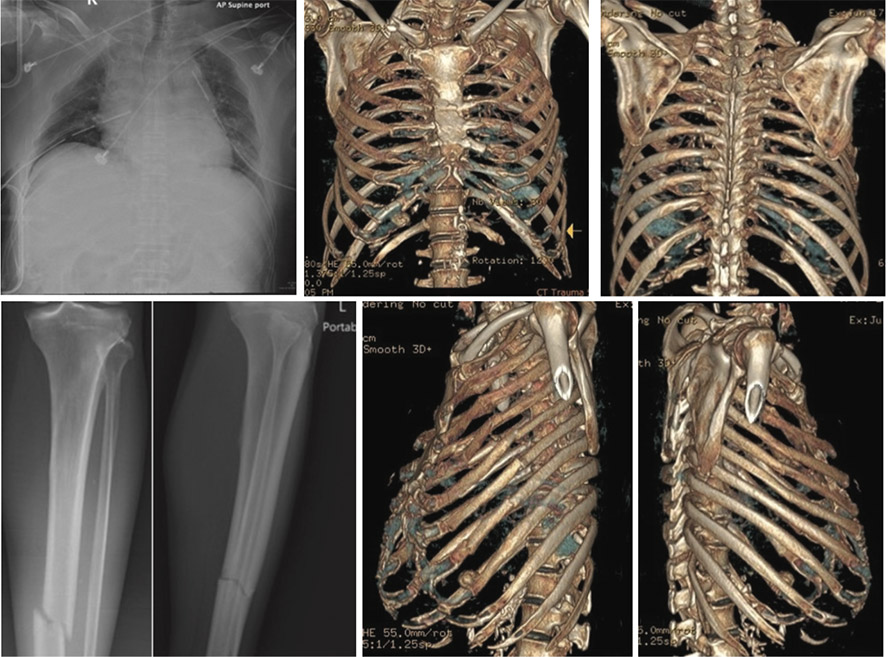
Figure 4
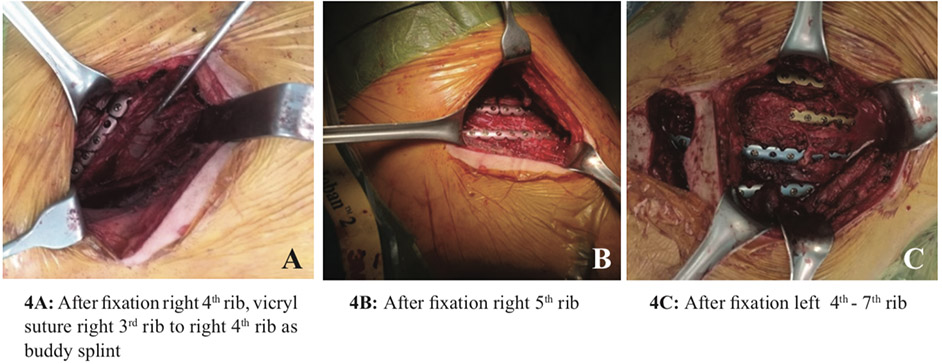
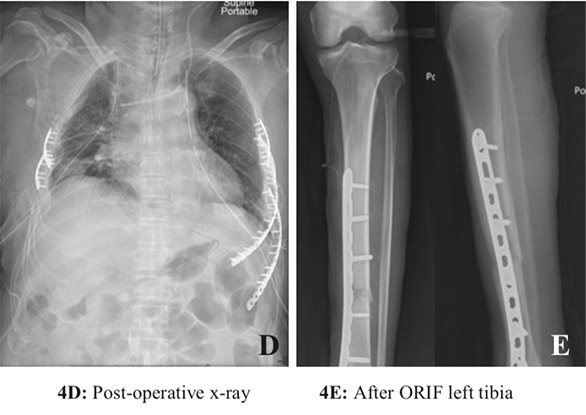
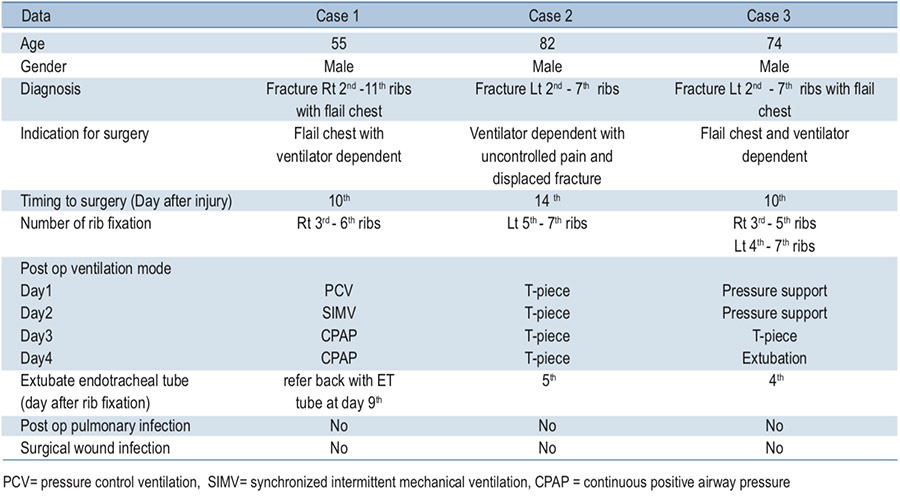
Table 1: summarized information of all cases
Multiple rib fractures and flail chest are common amongpatients sustaining blunt trauma. Due to the function of therib cage providing the mechanical support for the respiratorysystem and to protect intrathoracic organs, multiple rib fracturesor flail chest can compromise the respiratory systemwhich results in inadequate breathing, poor ventilation, reducestidal volume, and can lead to severe pain when breathingand also pulmonary contusion. These problems can leadto a prolonged ICU stay, prolonged intubation period, and agreater need of ventilator support.
Conservative treatment with analgesic medication, ventilatorsupport, and pulmonary toilet is the standard of care.6,7,10However, in some patients, especially in flail chest injury, thereis a paradoxical movement of the chest wall leading tomechanical failure of the bony structure of rib cage resultingin respiratory failure. Open reduction and internal fixation isan option in selected cases to improve mechanical structurefor respiration.
The advantage of rib fixation was shown in many systematicand meta-analysis reviews as detailed by Reinier B. Beks, etal.7 They suggested that rib fixation for flail chest could reducemorbidity compared to non-operative treatment. Furthermore,patients who underwent rib fixation had a shorter length ofstay in the ICU, shorter duration of mechanical ventilationand were diagnosed with a lower pneumonia rate.
In a study by Silvana F Marasco, et al.,1 a prospectiverandomized controlled trial was conducted to compare ORIFrib with mechanical ventilation management in flail chestpatients. The result revealed that the patients in the operatedgroup had a significantly shorter ICU stay and fewerrequirements for noninvasive ventilation after extubation.
In addition, Hafiz J Iqbal, et al.,11 also reported on theearly surgical stabilization in multiple rib fracture patients.They concluded that early surgical stabilization has a shorterICU stay and lower incidence of pneumonia. Most of theliteratures about rib fracture fixation reported the advantageof a shorter ICU stay, shorter intubation period, fewer pulmonaryinfections and shorter duration of mechanical ventilation inflail chest patients. However, in multiple rib fracture withoutflail chest there is insufficient data to support the advantage ofoperative fixation. Despite operative fixation in multiple ribfracture or flail chest having some advantages, the operationstill poses some risks including surgical exposure, iatrogenicpleural injury, infection or implant failure. We have to choosethe proper patients who fulfill the criteria for being suitablecandidates for rib fixation, as in our algorithm aiming toidentify the patients who will receive the most benefit fromfixation. In multiple rib fracture, the number of fixed ribs wasat the discretion of the surgeon, and depended on anatomicalboundaries and the possibility to regain stability of the chestwall during respiration.6,7 The suitability of a fixed fracturerib depends on several factors such as surgical exposure,fracture site and degree of displacement. Anterior and lateralrib fractures were preferentially fixed over posterior rib fractures,due to more reliable fixation and easier access comparedwith posterior rib fractures.1 In flail chest, usually addressedby fixing 1 fracture per rib, converting a flail segment tosimple fractured ribs is enough.1 In this report, we did not fixall of the rib fractures but we chose the most displaced andunstable ribs fracture segments with anterolateral approach toanterior or anterolateral rib cage with an easy to access fracturesite. In one skin incision (one window) we can expose and fix3-4 ribs per window.
In our report, with 1 skin incision (one window) we fixedonly 3-4 ribs in a multiple rib fracture and fixed at least 1fracture in flail chest injury. This was sufficient to stabilize thefracture segment, improve patient’s ventilation and reducepain. All of three cases in this report had satisfactory outcomeswithout complications. However, to fully validate the techniqueand the outcome shown in these reports, further study withmore cases is required.
To gain further insight of the outcomes, moreexaminations with more cases are required to fully understandthe benefits and risks of rib fracture fixation.
The main findings from the three patients demonstratedthat rib fracture fixation improved the quality of breathingwhich resulted in a short intubation period. The patientsshowed no sign of post-operative pulmonary infection. Withthe findings, the team suggested that rib fracture fixation is analternative choice of treatment for patients with flail chest.
The authors declare no potential conflicts ofinterest and there was no source of external funding for thisstudy.
The authors would like to thank Bangkok Health ResearchCenter for research assistance.









