Electronic ISSN 2287-0237
Chondroblastoma is rare, representing only 1-2% of all primary bone tumors and 5% of benign bone tumors.1 Most patients are under 20 years old. Chondroblastoma is usually located in the epiphysis or apophysis of long bones but it can occur in flat bones and vertebrae as well.1 Symptoms vary from mild to severe pain for periods followed by a decrease in range of motion. The standard treatment of chondroblastoma is tumor curettage with a bone graft.1 Management of chondroblastoma in the femoral head, however, is challenging due to the difficulty of access and the potential risk of damage to the epiphyseal plate. Radiofrequenct ablation (RFA) is a minimally invasive option for chondroblastoma management. Reports of a small series using this technique have been reported to have had excellent outcomes, but there is limited data on long term follow up.1-5
A 13-year old boy presented to the Orthopedic Out-patient Clinic in January 2012 with left hip pain and reported limping for 1 year. He also had night pain but no history of trauma to the left hip. His mother had brought him to a primary hospital where he was initially treated with NSAIDs but the pain did not subside. Physical examination at the Orthopedic Clinic revealed a left antalgic gait and tenderness at left groin with slightly limited internal rotation of the left hip.
Plain radiographs showed an eccentric well-circumscribed osteolytic lesion at the epiphysis of the left femoral head which measured 1.5x1.5 cm (Figure 1). Preoperative CT scans of the left hip showed a welldefined homogeneous osteolytic lesion 1.3x1.7x1.4 cm with a sclerotic border at the left femoral epiphysis (Figure 2). The inferior margin of the lesion was located on the epiphyseal plate of the femoral head while the superior margin was located beneath the articular surface.
Based on the pathology report, chondroblastoma of the left femoral head was diagnosed. To avoid risk of growth plate injury following open surgery, we chose percutaneous radiofrequency abrasion.
Informed consent was obtained and the protocol was approved by the institutional review board of our institute. The patient was placed in the supine position on a fracture table. Fluoroscopic drilling via the lateral approach was followed by Percutaneous Radiofrequency Ablation with a 70o Celsius monopolar probe for 3 minutes’ duration repeated 3 times performed in April 2012. A second ablation procedure was performed 3 months later in July 2012.
At the 3 months follow up visit in October 2012, the pain had significantly subsided and the patient could ambulate with partial weight bearing using an axillary crutch. At the 6 months follow up visit in January 2013; he could walk well without any gait aid and with only minimal pain even after long periods of walking. On further follow up visits between April 2013 and November 2016 he had no hip pain and enjoyed active sports. The follow up radiographs from each visit are shown in Figure 3.

Figure 1: showed eccentric well-circumscribed osteolytic lesion at epiphysis of left femoral head, which measured 1.5x1.5 cm.
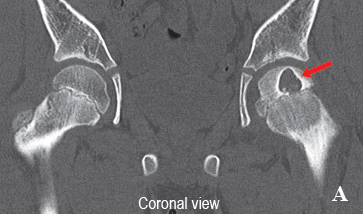

Figure 2: CT scan of left hip showed well homogenous osteolytic lesion 1.3x1.7x1.4 cm at left femoral epiphysis. The inferior margin of the lesion is located on the epiphyseal plate and the superior margin of the lesion is located on the articular surface.
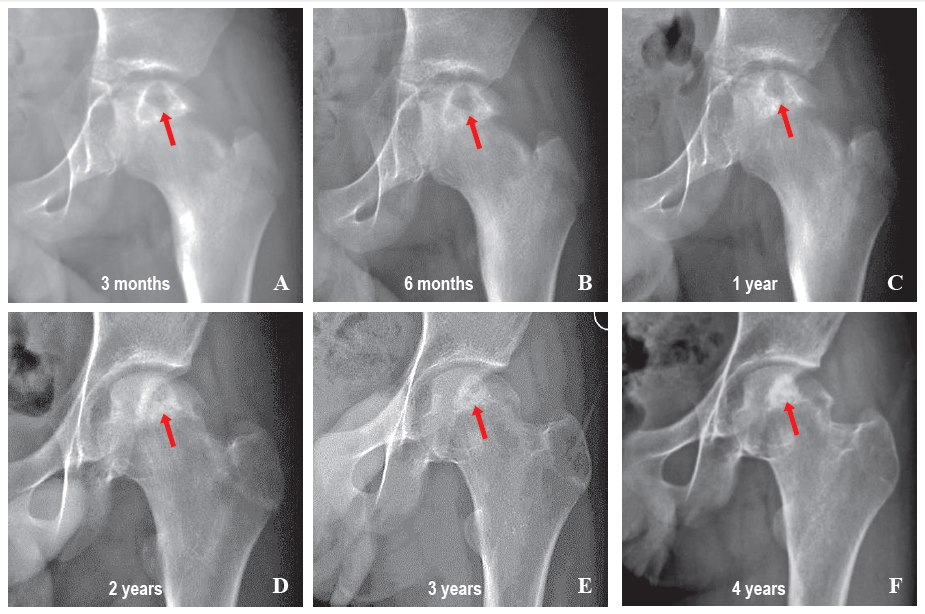
Figure 3: Follow up radiographs.
Chondroblastoma does not resolve spontaneously with conservative treatment. The mainstay treatment of chondroblastoma is entire tumor removal followed by filling the void defect. However, chondroblastoma in the femoral head requires special consideration because this area is difficult to access. Current options for treating this difficult lesion are complete tumor removal by open arthrotomy and tumor removal using minimally invasive procedures. Complete tumor removal can potentially result in femoral head collapse and growth plate damage, while minimally invasive procedures have the benefit of preserving the femoral head but present a risk of tumor recurrence.
Open surgery and tumor curettage of a femoral head lesion can be achieved through the base of femoral neck, trochanteric, or open hip arthrotomy approach.1,6 These techniques increase the risk of the tumor spreading to adjacent areas and of damaging the growth plate. Removal of the tumor from the articular cartilage side will cause femoral head collapse and late osteonecrosis of the femoral head. To prevent articular damage, hip arthroscopy can be used in combination with tumor curettage in a minimal invasive approach.1
Radiofrequency Ablation (RFA) as a minimally invasive procedure was introduced in 20012 and has increased in popularity since then. This technique minimizes the risk of mechanical collapse and growth plate injury and is suitable for small sized lesions. Several case reports have demonstrated that RFA can be applied to the periarticular area, especially the femoral head, proximal humerus, femoral condyle and tibial plateau.2-4,7,8
In difficult areas, such as the femoral head, several case reports and case series have shown that RFA has had excellent outcomes in terms of head preservation, no growth plate damage and no tumor recurrence (Table 1). The decision to treat with RFA is based on skeletal maturity and size of the lesion. In a skeletally immature patient, the largest tumor removed by RFA was 2 cm in diameter.8 In a skeletally mature patient, larger tumors can be accepted as there is no risk of epiphyseal plate injury. The largest tumor treated with this technique was 2.9 cm in diameter.7
In the present case, the patient still had bone growth remaining and the lesion was 1.7 cm in diameter. For those reasons, we selected RFA as the treatment of choice. The superior border of the lesion was the articular cartilage and the inferior border of the lesion was the growth plate. To prevent thermal injury to these structures, we chose RFA with a 70o Celsius probe for 3 minutes repeated 3 times. The heat and duration of each cycle were less than reported in previous studies. The lower heat and lower duration might result in local recurrence of the tumor, so we decided to perform a second operation using the same procedure 3 months later. The 3 months post-operative follow up found that the pain had subsided. At the 6 months follow up, he could walk without any gait aid. At the 3 years follow up, he had resumed playing soccer and bicycling. No subsequent complications were found in this case.
Complications of RFA can be classified as articular damage, growth plate disturbance or recurrence of the tumor. There have been no reports of any complications following femoral head RFA in previous studies, although complications in larger case series of RFA in periarticular operations have been mentioned. Rybak et al.4 and Lalam et al.3 reported articular surface collapse with the two largest sized tumors in their series (2.5x2.0x2.1 cm and 4.6x4.8x1.8 cm). Recurrence following radiofrequency ablation was mentioned in 1 of 17 cases reported by Rybak et al.4 and in 1 of 3 cases of Rajalakshmi et al.9 Using an alternative method for larger lesions, Petsas et al.7 treated two femoral head chondroblastomas with a combination of curettage and RFA with multitine electrodes (average tumor size 2.7 cm). They accessed the lesions via fluoroscopic drilling and partial curettage after which RFA was performed through the tract and a bone graft was inserted into the lesion. No complications or recurrences were reported with a mean follow up of 36 months.
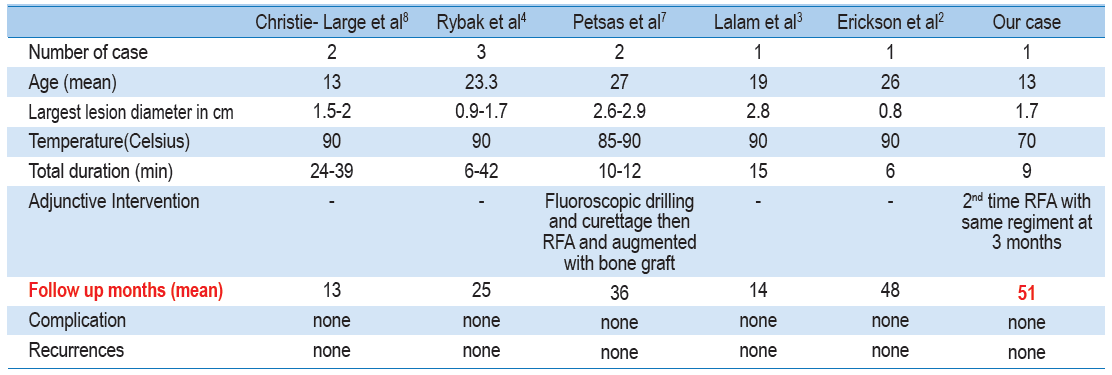
Table 1: Summary of the literature review of Chondroblastoma of femoral head treated with RFA.
Chondroblastoma of the femoral head in cases of skeletal immaturity is a challenge for the orthopedic surgeon. Adequate tumor removal might result in epiphyseal plate and articular damage, while minimally invasive treatment might allow recurrence of the tumor. Careful evaluation and risk-benefit analysis must be done before deciding on a treatment strategy. Fluoroscopic guidance for RFA is an excellent outcome Chondroblastoma of the femoral head in cases of skeletal immaturity is a challenge for the orthopedic surgeon. Adequate tumor removal might result in epiphyseal plate and articular damage, while minimally invasive treatment might allow recurrence of the tumor. Careful evaluation and risk-benefit analysis must be done before deciding on a treatment strategy. Fluoroscopic guidance for RFA is an excellent outcome
The authors thank Dr. G Lama Robert for helping us writing this manuscript.









