Electronic ISSN 2287-0237
Health literacy is an individual’s ability to understand and act on medical or health information and services in order to make appropriate health decisions. A growing body of evidence has shown that, compared to their counterparts, individuals with limited health literacy are less likely to use health care services appropriately,2-4 face difficulty following medical information,5,6 have a shorter life expectancy, and have worse physical and mental health.7 Specific to HIV, individuals with limited health literacy skills are more likely to possess inappropriate knowledge of their disease and its treatment, and have poor rates of medication adherence.5,8,9
The Institute of Medicine (IoM) recognizes that existing measures of health literacy are only approximations of reading skills framed within a broad healthcare context and development of a specific tool to better estimate patients’ understanding and capacity to understand health information and the true definition of health literacy is needed.1 Health literacy experts agree with the IoM and develop several instruments to assess health literacy both in general and in specific to diseases or health conditions, including HIV. Insert literature about health literacy tools and gaps in research here.10
We initially developed HIV-HLT from the literature review. This preliminary study aims to test its reliability and validity among people living with HIV.
Participants were recruited from the HIV clinic of Thammasat University Hospital in October 2019. This study was approved by the human research ethics committee of Thammasat University No.1, Faculty of medicine, (Protocol Approval No. MTU-EC-CF-0-099/62). The participants needed to meet all the inclusion and exclusion criteria listed below.
Inclusion criteria:
1. Both males and females
2. Age between 18 – 64 years old
3. Be diagnosed with HIV infection.
4. Being able to read, write and understand the Thailanguage.
Exclusion criteria: Participants had one or more of the following conditions, as noted in the medical record:
1. Cognitive impairment at any degree
2. Psychosis disorder
3. Memory impairment
4. Severely impaired vision not correctable with eyeglasses or blindness
5. Hearing problems uncorrectable with a hearing aid or deafness
Variables
Demographics data
Self-reported socio-demographic data included patient age, sexual orientation, marital status, family living, levels of educational attainment, occupations, income per month (baht), and medical scheme. Duration of HIV infection, CD4 count (cells/mm3) and viral load (copies/ml) were obtained through medical charts.
HIV health literacy
HIV health literacy was assessed with a HIV-HLT in Thai. The HIV health literacy questionnaire had two domains: HIV knowledge (10 items) and medication adherence (10 items). All interviews were conducted in a private room in the HIV clinic on the clinic appointment day before being seen by a physician.
Statistical analysis
Descriptive statistics were used to describe the percentage and frequencies. Principal components (PC) analysis was used to assess the construct validity of the 20-item scale. Corrected Item-Total Correlation is an index that ranges between 0 and 1. Corrected Item-Total Correlation of ≥ 2 was considered acceptable. Cronbach’s alpha was used to examine the reliability of derived HIV knowledge and medication adherence. The value of Cronbach’s alpha is an index that ranges between 0 and 1. A Cronbach’s alpha of 0.70 or higher indicates that items within the same scale measure the same underlying construct. All analyses were performed using SPSS version 22.0.
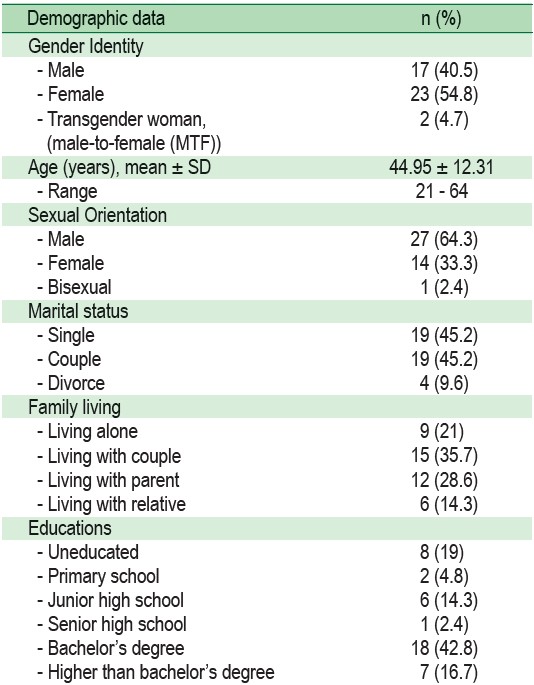
A total of 42 consecutive HIV infected patients were recruited to participate in the study. The participants (n = 42) had the mean age of 44.95 years (SD = 12.31 years), 40.5% were male, 54.8 % were female and 4.7% were transgender women, respectively. For the duration of HIV infection, 42.9% of the participants were diagnosed with HIV for more than 5 years. The majority of the participants had a CD4 count of >200 cells/cm3 and viral load of < 20 copies/ml (Table 1).
Table 1: Demographic data of participants (n=42)

The corrected item-total correlation of the 20 items was higher than 2, which was considered acceptable. The 20 items were further analyzed using PC analysis to assess validity, and Cronbach’s alpha was used to evaluate internal consistency.
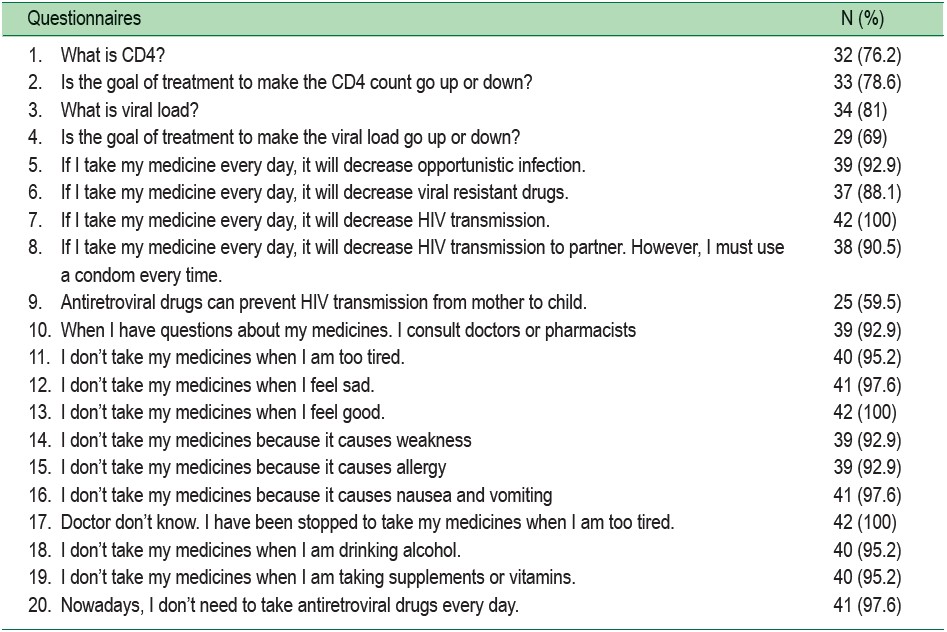
The scale had a Cronbach’s alpha of 0.89, which indicated that items within the same scale measured the same underlying construct (Table 2). More than 80% of participants responded correctly to 16 out of 20 items (Table 3)
Table 2: Association between HIV health literacy questionnaires, corrected item-total correlation and Cronbach’s alpha among 42 adults on treatment for HIV infection
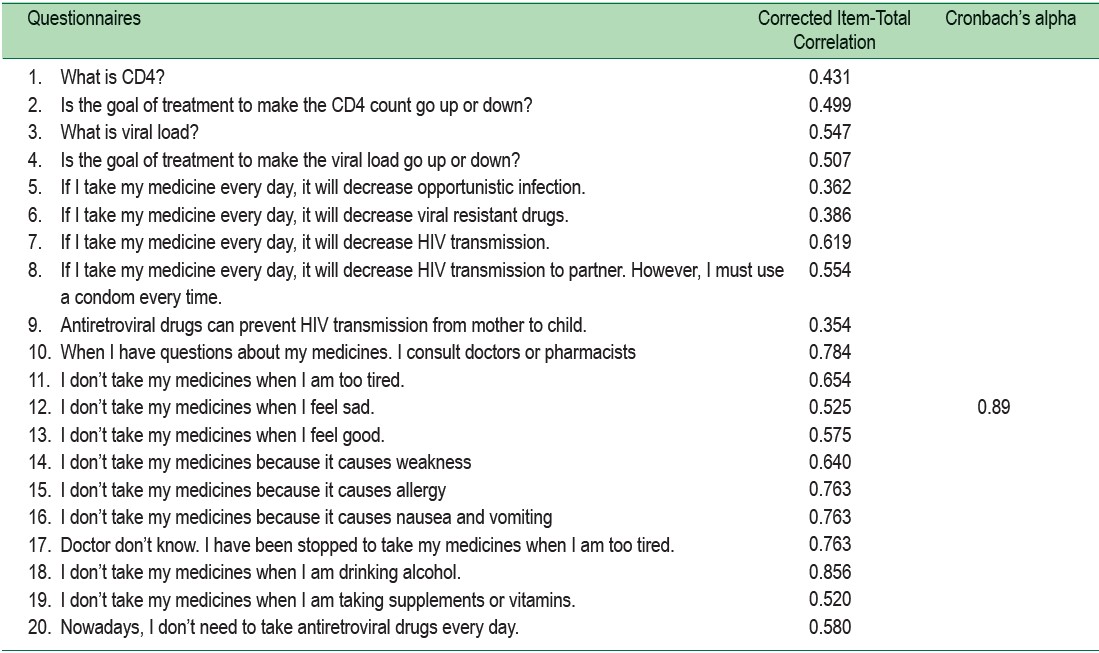
Table 3: Association between HIV Literacy items and correct responses among 42 adults on treatment for HIV infection (n = 42)
This study preliminarily tested the reliability and validity of HIV-HLT. Findings show that HIV-HLT was both valid and reliable for measuring health literacy among Thai patients living with HIV. This HIV-HLT is a novel instrument for HIV health literacy assessment. The study highlights several potential challenges related to patients’ ability to understand HIV information.
On previous studies of the development of HIV health literacy instruments, we found only two other similar studies conducted in sub-Saharan Africa measuring HIV literacy’s role in HIV related behaviors, knowledge, and outcomes. One recent study reported an association between limited literacy with lower HIV knowledge, and virologic suppression of HIV.11-13 Both studies applied suboptimal HIV health literacy measures since these were not specific to the HIV disease or health context of the studies.14
Participants had difficulty interpreting commonly used drugs, understanding the number of pills to take daily and correct time, and understanding discussed disease-related HIV concepts such as viral load, CD4 (T-lymphocyte) cell count, etc.11 The 20-items version of the HIV health literacy tool was also proven valid and reliable to measure HIV health literacy skills.
Identifying limited HIV health literacy is the first step in the development of strategies to access health information in HIV patients. For example, in the US, an intervention to improve communication of HIV-related information using pictograph-guided adherence counseling to HIV patients was developed for those with limited health literacy.15 This improved ART adherence and undetectable HIV viral loads, compared to HIV patients submitted to general health counseling. Improving health education materials, treatment instructions and simplifying commonly used prescription cards together with applying basic communication strategies such as the ‘‘teach-back/feedback model’’ are a few examples of interventions that can be used for those living with HIV.16-20
The HIV-HLT was designed to maintain items that assess HIV knowledge, medication adherence that can easily be used in the clinical setting to identify patients with limited health literacy skills. HIV-HLT is valid and reliable for Thai people living with HIV. The scale can be used for future research focusing on understanding the role of HIV health literacy as a mediator of HIV-associated behavior and health outcomes.
The reliability of HIV-HLT was only preliminarily studied due to the limited number of participants. Further investigation of the reliability of HIV-HLT among large participants is required.
This study was supported by a grant from Faculty of Medicine, Thammasat University, Pathum Thani Province, Thailand fund and facility support services from Thammasat Hospital University to S. Bunman is also acknowledged.









