Electronic ISSN 2287-0237
Physiological aging is inevitable and is characterized by gradualdeterioration of the body structure and function.1 Globally, however,life expectancy is increasing and, in many countries, fertility andmortality rates are declining. Consequently, the number and percentage ofolder individuals is increasing in nearly every nation.2 The World HealthOrganization estimated there were 600 million people aged 60 years and overin the year 2000.3 In 2017, it was estimated 962 million people aged 60 yearsand above in the world, comprising 13 percent of the global population.World Health Organization (WHO) projected 1.2 billion older adultsworldwide by 2025 and 2 billion by 2050.The global older population willbe 1.4 billion in 2030 and 2.1 billion in 2050, and as many as 3.1 billion in2100.4 The most rapid increases in the older population (140 percent by 2030)are occurring in developing countries.5 In the Kingdom of Bhutan in theeastern Himalayas, life expectancy has increased substantially, more thandoubling from 32.4 years in 1960 to 69.5 years in 2014, and it is projectedto be 75 by 2030.6 The number of adults 60 and older represents over 5% ofthe population and is expected to increase to 11.2% by 2045.7 With agingcome physical, psychological and social challenges for individuals,communities and societies. Studies in many nations have documented risingrates of problems such as fractures, osteoarthritis, other chronic diseases anddisability, dementia and hospitalization.8,9 In both modernized and developingcountries, therefore, it is vital to focus on not only longevity but also onhealthy longevity and quality of life. These, more than mere years lived, areessential components of successful aging.
Successful aging is a concept stressing the quality of aging.This term has been used interchangeably with terms such ashealthy aging, productive aging, and aging well.10 The conceptof successful aging has been interpreted from diverseperspectives, and while its definition has evolved throughresearch over the last 50 years, there remains no consensusdefinition.11,12 Generally, successful aging is characterized byhigh ability and function in the physical, mental, and socialdomains.13 Successful aging was proposed based on a theoryof adaptive development and effective life managementdomains. It incorporated behavioral, motivational, andcognitive processes in aging. Acknowledging decreasingcognitive function, the importance of adaptation strategiesthrough selective optimization with compensation has beensuggested.13 Successful aging concept was described bydifferentiating it from “usual” aging.14 Successful aging comprisesthree components: 1) avoiding disease and disability, 2)maintaining high cognitive and physical functioning, and 3)prolonging active engagement in life. 14,15
Successful aging is often defined as an individual’s“perception of a favorable outcome in adapting to the cumulativephysiologic and functional alternations associated with thepassage of time, while experiencing spiritual connectedness,and a sense of meaning and purpose in life”.16 Successfulaging occurs when an individual uses adaptive mechanismsand spiritual resources to achieve a balance between physicallimitations and environmental challenges.17 Successful agingcan include various factors such as perceived self-efficacy,social support, educational level, and perceived health statusand life satisfaction. However, despite the recognizedimportance of these factors, the relationship between them andsuccessful aging remains undefined.18,19
Perceived self-efficacy is, for older adults, a belief in theirability to control life-affecting events. Individuals with highself-efficacy will persevere, even in the absence of positiveoutcomes.20 Perceived self-efficacy shows a strong positivecorrelation with successful aging. Self-efficacy declines withincreasing age, and that decline is steepest in old age.21 Evenwith many of the problems associated with aging, however,a person with high perceived self-efficacy can accommodatehealth and functional declines and achieve successful aging.
Social support is also linked to successful aging, typicallycoming from family, friends and others with close relationshipswith the older person. Social support plays a meaningful rolein creating happiness, allowing older people to share agerelateddifficulties and to express love and affection. Researchhas found social support to be an essential factor in successfulaging.2,19
Educational attainment can affect health in different waysat different stages of the life cycle. Successful aging has beenhighly correlated with education, and evidence suggested thatthose with higher levels of education were more likely toengage in healthy behaviors and less likely to adopt unhealthyhabits.22,23
Older adults’ perceived health status has been linked toreduced risk of mortality, disability, depression, and bettercognitive health.24-27 High perceived health means individualsfeel better able to cope with changes that have occurred to theirbodies as they age, to deal overall with their aging, and topromote successful aging.16
Another key to successful aging is life satisfaction. Numerousstudies have found life satisfaction positively correlatedto successful aging. Education, lifelong learning activities, lifesatisfaction, and well-being were positively associated withsuccessful aging.28 Life satisfaction and the feeling ofbeing in control over one’s life are important aspects ofpsychological functioning in old age and have been discussedas important indicators of successful aging.13
Since there is no study about successful aging in Bhutan,therefore, we decided to study the predicting factors ofsuccessful aging among community dwelling older adults inThimphu, Bhutan. We expect that this study will help topromote successful aging among community dwelling elderly,in addition to increasing public awareness of the importanceof successful aging in Bhutan.
In this predictive correlational study, data were collectedwith 90 community dwelling participants living in fourvillages at Thimphu, Bhutan using convenience sampling fromApril to May, 2018. The selection criteria included:
Sample size was calculated following n = 50 + 8m (wheren is sample size, m is the number of independent variables).30Since this study has five independent variables, the minimumsample size was 90.
Research Instruments
Data were collected using six questionnaires.
Part 1: Demographic questionnaire. Constructed by theresearcher, this consisted of items measuring age, gender,marital status, educational level, income, co-morbidity,religion, and living arrangements.
Part 2: The General Self-Efficacy Scale (GSES). Thisscale, developed by Schwanrtzer and Jerusalem, 31 consists of 10 items, each scored on a four-point scale ranging from 1 (notat all true) to 4 (exactly true). GSES scores thus range from 10-40, with higher scores indicating higher self-efficacy.Cronbach’s alphas ranged from 0.76 to 0.90 with the majorityaround 0.80.
Part 3: The Multidimensional Scale of Perceived SocialSupport (MSPSS). Developed by Zimet GD, et al.,32 thisinstrument measures perceived social support from threesources: family, friends and significant others. The instrumentconsists of 12 items comprising three subscales: 1) Significantothers subscale items 1, 2, 5, 10, 2) Family subscale items 3,4, 8, 11., 3) Friends subscale items 6, 7, 9, 12. Each item is rated on a 7-point Likert scale (ranging from1 = very strongly disagree to 7 = very strongly agree). Internalconsistency coefficients for the three subscales were 0.69 forsignificant others; 0.78 for family and 0.76 for friends .33
Part 4: The Perceived Health Status scale. Self-rated healthwas used to measure perceived health status. This instrument,developed by the Stanford Chronic Disease Self-ManagementStudy, consists of 1 Likert scale item asking participants torate their general health, scored from 1 (poor) to 5 (excellent).Test reliability was 0.92.34
Part 5: Life Satisfaction Index for the Third Age-ShortForm (LSITA-SF). This is an updated and comparativelybriefer scale of 12 items based on the theoretical framework.35LSITA-SF scale reliability was 0.90 with satisfactory content,construct and criterion validity. This short version measuresonly the overall construct of life satisfaction. Each item scoreranges from strongly disagree to strongly agree. Reversescoring is used for some items.
Part 6: The Successful Aging Inventory (SAI). Thisinstrument, developed by Troutman,36 based on theory,37consists of 20 items, each a brief, positively worded statementexpressing a single idea or behavior suggestive of successfulaging. Items are rated on a 4 point Likert scale (from 0 =hardly ever/ strongly disagree to 4 = almost always/stronglyagree). Higher scores indicate more successful aging.Cronbach’s alpha coefficient was 0.86.
The original versions of all instruments were translatedinto Dzongkha, the Bhutanese language. The back translationprocess was used to ensure content validity of the questionnaires.38Then the Dzongkha versions of all instruments were tested bya pilot test for internal consistency using Cronbach’s alpha.Reliability was tested on 30 older adults in Thimphu, Bhutanwith characteristics similar to the samples. Cronbach’s alphafor GSES, MSPSS, LISTA-SF and SAI were 0.90, 0.90, 0.70and 0.70, respectively.
Ethical considerations
This study was approved by the Human Research EthicsCommittee of Faculty of Nursing, Burapha University(approval 07-02-2561) and the Research Ethical Board,Ministry of Health, Bhutan. This is to protect the rights of thesamples, starting from the data collection process until thefindings of the research are presented. The researcher explainedclearly the purpose of the research and research procedures,and notified the participants of their rights regardingwithdrawal from the study, which stipulates they can withdrawanytime without any negative effects.
Data collection procedure
Researchers visited participants who met inclusion criteriaat their home. Firstly, they were screened with the Six ItemCognitive Impairment Test. If they passed the test, then theresearcher explained and administered those 6 questionnairesin Dzongkha. Each interview took 40-50 minutes. Interviewswere conducted between 9 a.m. and 5 p.m. everyday. Theresearcher finally collected the data from 90 cases as planned.Data analysis
Characteristics of the sample are shown in Table 1. Mostof the participants (58.9%) were female, all (100%) wereBuddhist, and half were young-old (52.2% age 60-69, mean= 70.43, SD = 7.53). Half (51.1%) had no formal educationand half (50.7%) were married. Almost three-quarters (72.2%)were living with their families. Half (50%) had no currentillness and most (83.3%) had no income. Summary statisticsfor the variables used to measure variables are shown in Table 2.The mean score of perceived self-efficacy was 31.58 (range =10-40, SD = 8.49). The mean score for social support was74.87 (range = 12-84, SD = 12.46). The mean educationallevel score was 1.18 (range = 0-18, SD = 1.63). The meanperceived health status score was 2.59 (range = 1-5, SD =0.75). The mean life satisfaction score was 47.07 (range =16-68, SD = 8.56). The mean successful aging score was 69.78(range = 27-80, SD = 11.72).
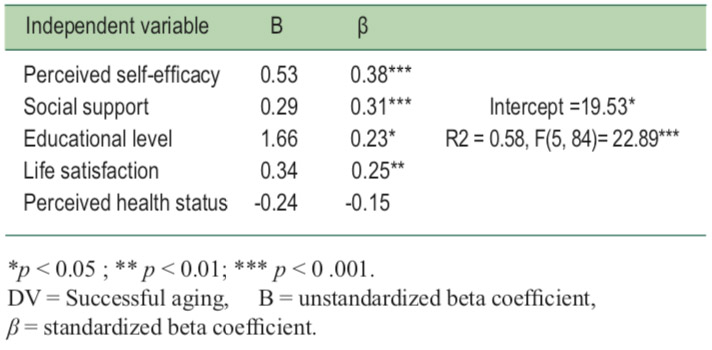
Correlations between the dependent variable of successfulaging and the five predictors. Perceived self-efficacy, socialsupport, life satisfaction and educational level were allpositively and significantly (p < 0.001) related to successfulaging. Perceived health status was not related to successfulaging see Table 3. Multiple regression analysis showed socialsupport, life satisfaction and perceived self-efficacy, andeducational level significantly explained successful agingaccounting for 58% of the variance in successful aging(R2 = 0.58, F(5, 84)= 22.90, p < 0.000) see Table 4.
Table 1: Characteristics of the samples (n = 90).
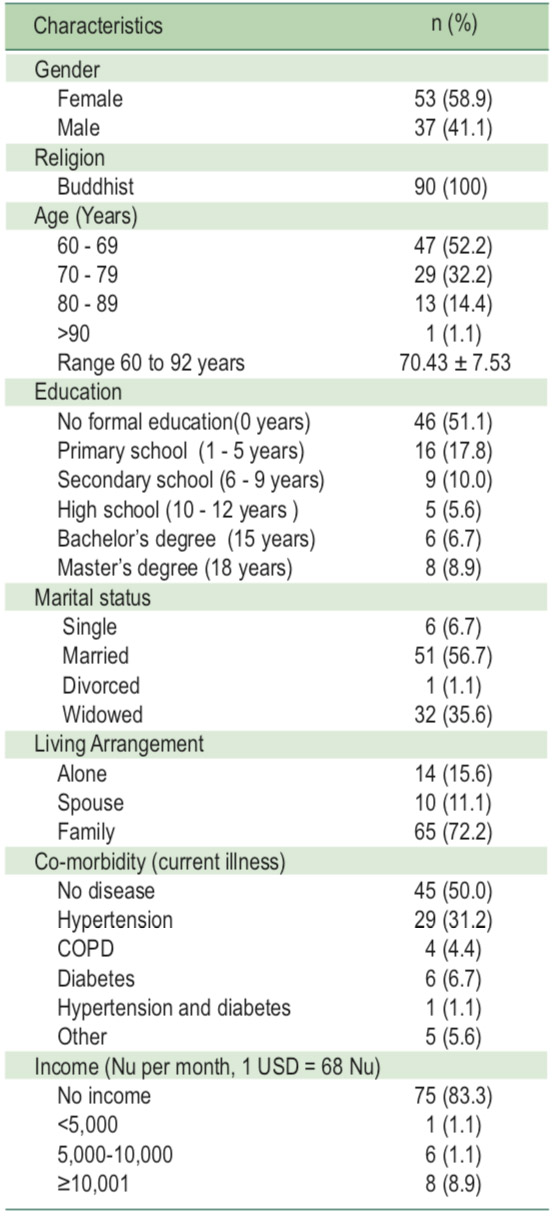
Table 2: Descriptive statistics of variables.
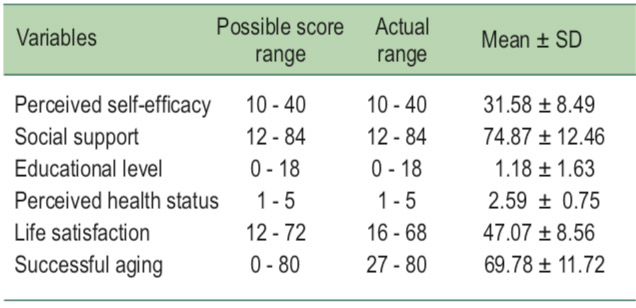
Table 3: Correlation coefficients for perceived self-efficacy, social support, life satisfaction, educational level, perceived health status, and successful aging.
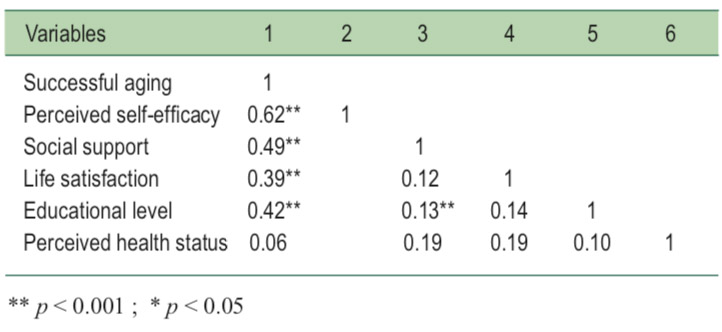
Table 4: Predicting factors of successful aging
This study hypothesized that high levels of five factors―perceived self-efficacy, social support, education, perceivedhealth status, and life satisfaction―could predict successfulaging among community dwelling older adults living inThimphu, Bhutan.
First, perceived self-efficacy was a significant correlateand predictor of successful aging (r = 0.62, p < 0.001);β = 0.38, p < 0.001). According to successful aging theoriesdiscussed above, more perceived self-efficacy meant greaterpersonal control, creativity, and confidence. People withhigher self-efficacy ostensibly have more knowledge andexperience to cope with any type of change, includingphysiological, psychological, and social changes that typically accompany aging. Higher self-efficacy improves theodds of finding thoughtful, innovative solutions to age-relatedchallenges.37 It should be noted that just over half of the olderadults in this study were young-old (age 60-69). Among theolder population, this age group is most likely to be active,healthy, independent, socially engaged and able to cope withthe modern accoutrements of contemporary life. This findswidespread research support. It was found that high perceivedself-efficacy contributed to happiness, life satisfaction, positivebehaviors, willingness to face challenges, emotional balance,and decreased stress.39 It was reported in similar findingsregarding perceived self-efficacy and successful aging.2,19,40In addition, low perceived self-efficacy may lead to giving upcertain behaviors or activities once challenging circumstancesarise.41 High perceived self-efficacy is thus a logical and crucialfactor in successful aging, determining whether older adults can or are willing to try to meet age-linked threats totheir well-being and quality of life.
Second, several studies have found social supportsignificantly related to successful aging. The same was foundamong older community-dwelling adults in Thimphu, Bhutan(r = 0.49, p < 0.001); β =0.31, p < 0.001). Over 70% ofparticipants were living with family, where intergenerationalsupport, especially flowing from younger to older generations,is a strong cultural norm and can contribute to successfulaging. Filial piety, where the younger generation respects andsupports their older family members, is an expectation inseveral Asian cultures. Family is an important provider ofsocial support for older adults and can provide them withconfidence, goals and goal attainment, higher motivation andlifelong experiences. The notion that social support is significantlyrelated and can predict successful aging is supported.2,19,39,42
Next, in this study educational level was a statisticallysignificant correlate and predictor of successful aging in thissample of older adults (r = 0.42, p < 0.001; β = 0.23, p < 0.05).Education can be a significant facilitator of achieving goals,including health and physical functioning,43 which can lead togreater perceived self-efficacy and thus greater odds ofsuccessful aging. In this study, though, 51% of participantshad no formal education and another 18% had five years ofless of education. This may be due to the uniqueness ofBhutanese that focus on gross national happiness. Therefore,even they have low educational level, they are happy and livesuccessfully. However, it was found that higher educationallevel was not associated with successful aging.44
High perceived health status has been related to lower riskof mortality and reduced disability.45 But as age increases,health typically worsens; the studies found a negativerelationship between health and age.46 Yet in this study,contrary to these and other studies, and thus the testedhypothesis, perceived health status was not a correlate orpredictor of successful aging (r = 0.06, p > 0.05; β = -0.15,p > 0.05). It is possible that this could be due to samplehomogeneity on some variables. For example, half theparticipants were age 60-69 and more likely to perceive theirhealth as good. Half had none of the health problems measuredin this study. Nearly three-quarters lived with family who couldassist them, possibly obscuring health problems from theolder adults or allowing them to deny them, which would leadthem to perceive their health as better than it really was.There can also be, with increasing age, a shift inmetaperspective, from a materialistic and rationalistperspective to a more mature and existential one wheretranscending experiences are more likely (e.g., lower deathanxiety, more wisdom). Consequently, physical health maydecline in importance compared to, say, spiritual health. Thiswould be consistent with criticisms of Rowe and Kahn’smodel,14,15 i.e., that disease or disability disqualify one fromaging successfully.
The last independent variable, life satisfaction, was astatistically significant correlate and predictor of successfulaging (r = 0.39, p < 0.001; β = 0.25, p < 0.05). Life satisfactionis one’s evaluation of life as a whole, rather than the feelingsand emotions that are experienced in the moment. It can beargued that when older adults are satisfied with their lives, theyare more accepting of death, they may increase both religiosityand religious practice, they are more likely to engage inregular physical activity or exercise to improve or maintaintheir health, they are more likely to monitor their diet, theywill be more positive, and they will feel more autonomous; allof these are linked to successful aging. It was found that majorityof respondents identified life satisfaction as leading tosuccessful aging.47 Koltko-Rivera48 has proposed thatsubjective wellbeing in later life may be perceived as abuilding block process similar to Maslow’s self-actualizationhierarchy. Subjective well-being requires the fulfillment oflower needs (life satisfaction) before the individual can reachthe higher level needs of self-actualization (successful aging).
This is first study of its kind in Bhutan. Most of the findingswere consistent with prior research: it can thus be argued thatperceived self-efficacy, social support, educational level andlife satisfaction can predict successful aging in Bhutan.Nurses and health care providers should focus on these factorswhen providing care to enhance successful aging in olderadults. More study is needed, however, on the relationship ofperceived health status to successful aging among Bhutaneseelderly. There is a strong (but not universal) consensus aboutthe relationship, but it was not a statistically significant one inthis study. Nursing intervention regarding perceived healthstatus, perceived self-efficacy, and social support should bedesigned and researched in order to promote and enhancesuccessful aging for older adults as well.









