Electronic ISSN 2287-0237
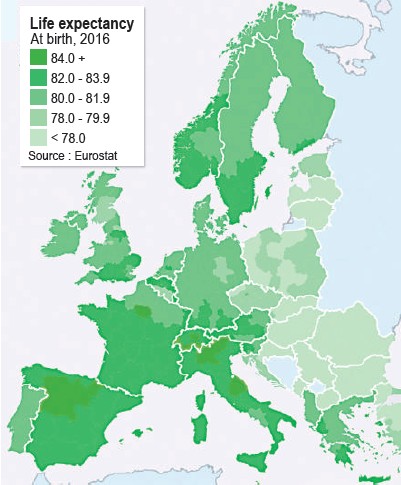
Anno 2019 cardiovascular diseases (CVD) remain the most importantcauses of death worldwide. Nearly 18 million people die from CVDper year according to the World Health Organization (WHO). Alsoin “Europe” CVD remain the most important cause of death. The latest datafor life expectancy at birth in Europe are shown in Figure 1. The moststriking overall difference between countries is the much lower life expectancyin the Eastern part of Europe. This difference can for a significant part beexplained by a much higher CVD mortality in Eastern Europe. Explanationsfor other differences e.g. those between West-European countries and thosewithin countries are not so obvious. In this paper we will describe importantchanges in risk factors, causes of death and mortality that took place inEurope in recent years and what can be expected in the near future.
Comparisons with other regions in the world will occasionallybe made. “Europe” in this paper is usually defined as the 53members states according to the WHO (www.who.int) or the57 member states of the European Society of Cardiology (ESC):most countries according to the WHO and, in addition, mostcountries bordering the Mediterranean sea (see be website ofESC: www.escardio.org).
The most important forms of CVD are ischemic heartdisease (IHD) and stroke. If CVD data are discussed theycomprise all forms of CVD. Occasionally data on IHD andstroke are provided separately. Many data discussed in thisdocument come from the World Health Organization (WHO),World Bank and the Institute for Health Metrics and Evaluationand were analyzed by the ESC Atlas group and reported in aspecial article in the European Heart Journal1.
Blood pressure, cholesterol levels, diabetes and smokingstatus are the most important risk factors for CVD. This isnicely illustrated in a long-term US study: participants in thestudy who were 55 years of age and who had an optimal riskfactor profile (defined as total cholesterol < 180 mg/dl, bloodpressure < 120/80 mm Hg, nonsmoking and nondiabeticstatus) had a substantially lower risk of death from CVDthrough the age of 80 years (figure 2A and 2B)2. When welook at these risk factors in Europe important observationscan be made. The prevalence of raised blood pressure overallis higher in men than in women and higher in the eastern partof Europe for both men and women. Between 1980 and 2014systolic blood pressure in ESC member states came downfrom 134 to 120 mmHg in women and from 138 to 130 mmHgin men. In 2014 mean systolic blood pressure was lowest incountries with a high income.
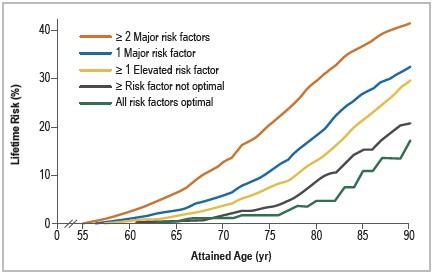
Figure 2A: Lifetime Risk of Death from Cardiovascular Diseaseamong Black Men and White Men at 55 Years of Age, Accordingto the Aggregate Burden of Risk Factors and Adjusted forCompeting Risks of Death.2
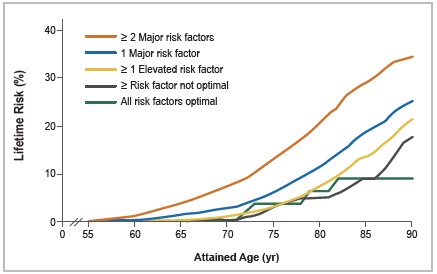
Figure 2B: Lifetime Risk of Death from Cardiovascular Diseaseamong Black Women and White Women at 55 Years of Age,According to the Aggregate Burden of Risk Factors andAdjusted for Competing Risks of Death.2
Cholesterol is a major target of risk reduction andglobally 33 % of IHD can be attributed to hypercholesterolemia.In general hypercholesterolemia is most common inhigh-income countries, thus in the Western world. Between1980 and 2009 mean cholesterol levels declined from 217 to197 mg/dl in the ESC member states. The incidence ofhypercholesterolemia was 18.9 % and 19.0 % in women andmen in high-income countries and 12.0 % and 10.0 %respectively in middle-income countries. A greater decline ofcholesterol levels was found in high income countries.
It is estimated that > 25% of all Europeans are smokers.The prevalence of smoking ranges from < 15% in someScandinavian countries to > 50 % in countries of the previousSoviet Union. Between 1995 and 2014 the average prevalenceof smoking declined from 21.4 % to 16.1 % in women andfrom 37% to 16.9 % in men (data from only 28 and 27countries in women and men, respectively). It is very importantto distinguish the acute and long-term harm of smoking.Obviously smoking enhances the development of atherosclerosisbut smoking has also a strong pro-thrombotic effect. When asmoking ban was introduced in public places and restaurantsin Western European countries, already after a few months asignificant reduction in the incidence of acute myocardialinfarction was observed which is difficult to explain by aneffect on the development of atherosclerosis .The disappearanceof the pro-thrombotic effect of smoking, which occursimmediately after smoking cessation, most likely explains thestriking reduction in the risk of acute myocardial infarction.
It is estimated that the prevalence of diabetes in 2014 isaround 6.5% in the ESC countries. Most of these cases aretype 2 diabetes. In 2014 Egypt, Lebanon and Turkey had thehighest prevalence (16.6, 14.9 and 14.8 %, respectively).Much lower rates (< 3 %) were found in some poor EasternEuropean countries (e.g. Moldova, Georgia, Armenia). In thetime frame 1995-2000 to 2014 the average prevalence ofdiabetes increased in both middle-income and high- incomecountries. Data on obesity are more or less in line with thoseon diabetes. E.g. female obesity was most common in Turkeywhere one in three women is obese.
Behavioral factors such as alcohol consumption and lackof physical exercise do have an impact on CVD and shouldbe also be considered as risk factors. In subjects > 15 yearsof age in ESC member states for which data are available theaverage alcohol consumption averaged 8.7 L/capita/year(calculated as amount of pure alcohol in liters consumed overa calendar year). Large differences were observed with thehighest consumption in countries that were part of the previousSoviet Union and the lowest consumption in countries with alarge Islamic population. Little change in alcohol consumptionwas found between 1996-2000 and 2014. Insufficient physicalactivity in adults in ESC member states, graded viaquestionnaires is estimated at 30.1% in women and 22.7% inmen across the ESC member states. In general physical activitywas higher in middle-income countries as compared tohigher income countries. Physical inactivity is becoming amajor problem in Western countries. In high-income ESCmember states participation in at least 1 hour of moderate tovigorous physical activity per day among children aged 11,13 and 15 years was 20,14 and 9% in girls and 29, 23 and19% in boys. Much higher percentages were observed inmiddle-income countries, especially in boys.
Mortality as reported by the ESC Atlas of Cardiology
In global terms citizens of the EU live 2.5 years longerthan in the US and 4.6 years longer than in China. In a largereport from the ESC Atlas mortality data from 47 of 56 ESCmember countries were collected and analyzed1. Thesereported mortality data are the most recent ones but in somecountries (7/47) they date from 2010 or even before. Also thequality of the data varies between countries. The latestavailable data indicate that CVD is responsible for almost 4million deaths each year in the ESC countries (45% of alldeaths). CVD accounted for a larger proportion of all deathsin women (49%) compared with men (40 %). Stratificationby national income indicates a much lower CVD mortality inhigh income countries vs middle or low income countries.After CVD, cancer was the next most common cause of deathaccounting for 23% of all deaths. Importantly, in high incomecountries (Belgium, Denmark, France, Italy, Luxembourg,Netherlands, Norway, Portugal, Slovenia, Spain and the UK)cancer has become the most common cause of death in men.In women this is only the case in Israel and Denmark.More meaningful comparisons between countries can bemade with age-adjusted mortality rates (removing impact ofdifferences in population age structure). The averageage-standardized mortality rates for IHD across ESC membercountries (using data from 2014) were 241 per 100 000 inwomen and 384 per 100 000 in men. Using the latest availabledata, the countries with the highest rates were Belarus,Kyrgyzstan, Republic of Moldova, Russian Federation, andUkraine with rates of > 500 for women and > 800 for men.At the other end of the spectrum, countries with the lowestrates were France, Luxembourg, the Netherlands, Portugal,and Spain where rates were < 60 in women and < 120 in menper 100. Age-standardized stroke mortality (latest availabledata 2014), averaged across ESC member countries, wassimilar between women and men (133 and 173 per 100 000people). For individual countries, rates ranged from < 55 per100 000 women and < 60 per 100 000 men in France, Israel,Luxembourg, and Switzerland (as well as women in Spain)to > 300 per 100 000 people for both sexes in Bulgaria,Kyrgyzstan, Russian Federation, and North Macedonia (alsomen in Republic of Moldova).Temporal changes by national income status: Completeprevalence data for IHD mortality across three time periodsbetween 1985 and 2014 were available for 38 ESC membercountries. During that period, the average age-standardizedmortality due to IHD declined from 374 to 209 deaths per100 000 in women and from 586 to 339 deaths per 100 000in men. All of the 27 high-income countries for which datawere available recorded a decline in IHD mortality, averaging286 to 129 deaths per 100 000 in women and 508 to 227 deathsper 100 000 in men. In middle-income countries, the averagemortality also declined during this period in both women (591to 405 deaths per 100 000) and men (779 to 614 deaths per100 000). At a national level, however, the pattern wasinconsistent and while many countries showed variable reductionsin IHD mortality, it increased in Kyrgyzstan and Bosnia andHerzegovina in both women and men and also in men fromUkraine. There have been similar trends in age-standardizedstroke mortality, with steady declines occurring since the1980s in most high-income ESC member countries and morerecent declines in middle-income countries. Trends inpremature (< 65 years) IHD and stroke mortality have alsobeen similar, with consistent declines in the high incomemember countries of the ESC, and more volatile trends inmiddle income countries.
The interplay of healthy life style, socioeconomic statusand quality of health care
In high-income countries a healthy life style and a wellorganizedhealth care system are responsible for a significantdecline in CVD mortality over the last 40 to 50 years. In astudy performed on US data, the causes of the decline inmortality from coronary heart disease between 1980 and 2000in adults was examined. In this study it has been estimatedthat approximately half of the observed decline in mortalitymay be attributable to reductions in major risk factors andapproximately half to evidence-based therapies3 (Figure 3).This is probably also the case in Western European countries.As a result of the sharp decline in CVD mortality, cancer hasbecome the main cause of death in some of the WesternEuropean countries (cfr supra). However, within these countriesdifferences in life expectancy (and in CVD mortality) betweenregions still exist (e.g. Belgium North vs South, France Northvs South, Germany West vs East). Similarly large disparitiesin total burden of CVD persist between US states4. They canbe explained for a great part by differences in socioeconomicstatus and an associated different exposure to known riskfactors. However socioeconomic status cannot explain alldifferences in life expectancy and CVD mortality. An extreme example in this regard is the surprising observation that lifeexpectancy today in the US and in Cuba is more or less thesame in spite of the fact modern high tech procedures cannotbe performed in most places in Cuba. The lack of high techmedicine in Cuba is probably compensated by an excellentfree health system focused on prevention. It is only when life style (primary prevention), health care (evidence basedmedicine) and socioeconomic status (income and socialsecurity) are all three optimal in the total population of acountry that a (very) low CVD mortality and a (very) highlife expectancy can be expected. Examples are Japan,Switzerland, Sweden, and Australia.5 (Figure 4).
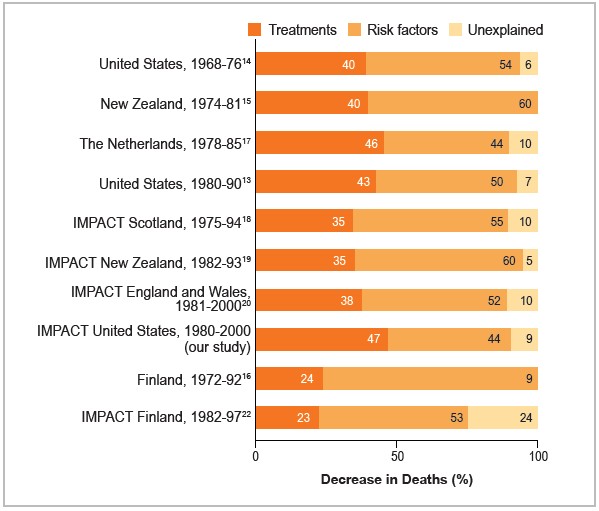
Figure 3: Decrease in Deaths from Coronary Heart Disease Attributed to Treatments and Risk-Factor Change.6
Figure 4: Health Care Spending in the United States and Other High-Income Countries.5
The cost of health care
It has been estimated that the annual cost of CVD to the EUcommunity (28 countries belonging to the European Union) isaround 169 billion per year. Similar data from other Europeancountries are not available or less reliable. However, it has alsobecome clear that implementing a healthy life style and offeringoptimal health care for all citizens is expensive, and the reasonwhy both can only be achieved in high income countries. Inaddition, an important evolution has taken place since thebeginning of this century. Severely ill and increasingly elderlypatients with very complex conditions are now being treated withsophisticated therapies (e.g. a patient in cardiogenic shock beingtreated with ECMO, left ventricular assist devices, heartPredicting CVD mortality globally and in EuropeIn a recent article published in The Lancet, a forecast of lifeexpectancy, years of life lost (YLL) and all cause andcause-specific mortality in 2040 for 195 countries and territoriesis presented8. Remarkable differences between super-regionswere found (Figure 6). Important changes are forecasted in Southand Southeast Asia. In these regions, life expectance isexpected to increase from 63.6 years in 1980 to 79.8 years onaverage in 2040 with non-communicable diseases (for a greatpart CVD and cancer) becoming the most important cause ofdeath (83.2%). A similar trend is predicted in central andEastern Europe while in Western Europe (high income countries)smaller shifts are forecasted (predicted life expectancy increasefrom 73.7 in 1980 to 82.5 years on average in 2040 withnon-communicable disease becoming the cause of death in85.7 % of the cases.transplantation in patients above the age of 65 years etc.). As aresult improvements in CVD mortality are obtained at very high(unsustainable?) increases in cost. A nice example in this regardare the data from 200 years of hospital costs and mortality of awell-known hospital (Massachusetts General Hospital)published in the New England Journal of Medicine7(Figure 5). The authors of this article conclude that improvementsin in patient mortality may be coming at unsustainableincreases in cost. This may even be a greater problem in the nearfuture with the development of new treatments for cancer whichhas become the number one cause of death in some Westerncountries (cfr supra).Treatments with proton therapy andimmune therapy are extremely expensive and the survivalbenefit so far has been modest.
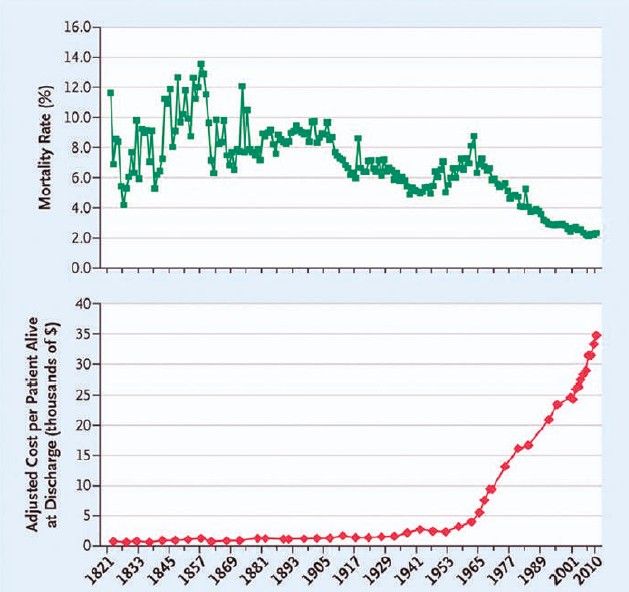
Figure 5: Two hundred years of hospital costs and mortality.7
Predicting CVD mortality globally and in Europe
In a recent article published in The Lancet, a forecast of lifeexpectancy, years of life lost (YLL) and all cause andcause-specific mortality in 2040 for 195 countries and territoriesis presented8. Remarkable differences between super-regionswere found (Figure 6). Important changes are forecasted in Southand Southeast Asia. In these regions, life expectance isexpected to increase from 63.6 years in 1980 to 79.8 years onaverage in 2040 with non-communicable diseases (for a greatpart CVD and cancer) becoming the most important cause ofdeath (83.2%). A similar trend is predicted in central andEastern Europe while in Western Europe (high income countries)smaller shifts are forecasted (predicted life expectancy increasefrom 73.7 in 1980 to 82.5 years on average in 2040 withnon-communicable disease becoming the cause of death in85.7 % of the cases.
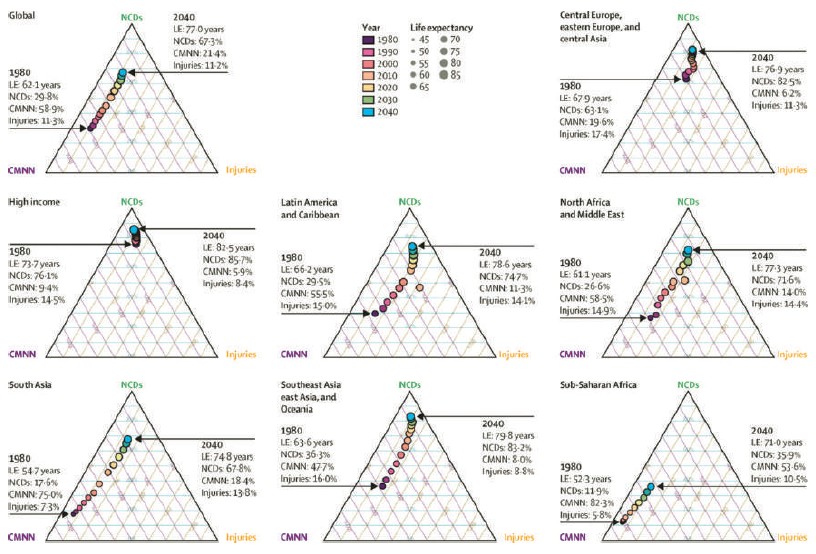
Figure 6: Forecasting life expectancy, years of life lost, and all-cause and cause-specific mortality for 250 causes of death:reference and alternative scenarios for 2016-40 for 195 countries and territories.8
Life expectancy in South and South-East Asia will increasein the next decades. Non-communicable diseases will becomethe main cause of death as in Western countries. Preventivemeasures will be critically important to avoid a large transientincrease in CVD mortality in the next decade In addition anaffordable and guidelines recommended health care systemfor all citizens will be needed to get life expectance figuressimilar to those currently seen in West European countries.









