Electronic ISSN 2287-0237
Headache is one of the most common problems that bring patients to the neurology clinic. Several precipitants can trigger headaches such as laughing, coughing, straining, sneezing, stooping, or sexual activity.1 Here we described an atypical presentation of headache onset after laughter in one patient.
A 50-year-old man visited the Comprehensive Headache Clinic at Bangkok Hospital Medical Center with the chief complaint of headaches occurring when he was laughing.
For the past thirty years, he had suffered from severe occipital pain provoked by laughing. He described the abrupt onset of sharp shooting pain at posterior part of upper cervical area, which radiated to bilateral occipital areas after vigorous laughing. The attacks lasted anywhere from a few seconds to a few minutes and were followed by a throbbing sensation at the same area which resolved spontaneously in less than an hour. The attacks only occured after laughing. Coughing, valsalva-like maneuver, straining when passing stool, change of position, or bending of neck could not precipitate headache or neck pain. He had no associated symptoms such as nausea, vomiting, photophobia, phonophobia, dizziness, fainting, blurring of vision, ptosis, lacrimation, conjunctival injection, or rhinorrhea during the attacks.
His past medical history was otherwise unremarkable. He denied history of head and neck injury, or chronic illness. Family history was unremarkable. No family members ever had headaches.
The neurological examination revealed normal cranial nerves function, normal motor power, no sensory loss, normal reflexes and normal gait. Neck examination showed mild restriction of range of motion both on flexion and extension, mild tenderness and spasm of upper posterior neck muscles, mild to moderate tenderness of occipital nerve area on both sides. Valsalva maneuver, coughing, and changing position (from lying to sit up and vice versa) was tried but could not provoke neck pain or headache.
Secondary cause of headache and neck pain was suspected. MRI of cervical spine including the posterior fossa was performed. MRI demonstrated Arnold-Chiari type I malformation (ACM), syringomyelia at C-3 level, and mild intervertebral disc bulging (Figure 1).
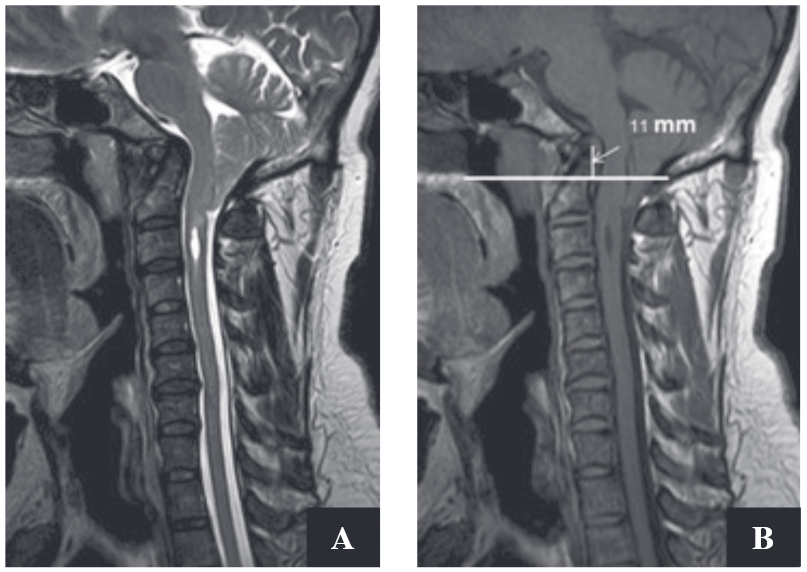
Figure 1A-B: Sagittal T2W (A), and T1W (B) show downward displacement of the cerebellar tonsil at the posterior foramen magnum. There is high signal T2W of cavitary syrinx in cervical cord demonstrated in (A). The basilar invagination is also demonstrated as protruded dens with the tip at 11 mm. above theChamberlain line (B).
Neurosurgical consultation was done. Posterior fossa decompression was recommended but the patient refused the operation.
Laughing induced headache is a rare presentation in headache clinics. To our knowledge, laughing induced headache was rarely reported in the literature.2-4 In 1956, Sir Charles Sydmonds reported 27 patients with transient severe head pain provoked by coughing, sneezing, straining at stool, laughing or stooping.5 International Classification of Headache Disorders (ICHD) II criteria do not include laughing headache.6 However in the symptomatic cough headache as described in Pascual’s series, head pain could also be precipitated by laughing.7
Cough headache can be induced by laughing, weight lifting, sudden postural change of head or body in addition to cough. Secondary cough headache has been described in hindbrain anomalies, including the Arnold-Chiari type I malformation.7 Chiari I malformation is a congenital disorder characterized by abnormal extension of the cerebellar tonsils below the foramen magnum and is sometimes accompanied by rostral displacement or exten- sion of the medulla. Patients with Chiari I malformation are often asymptomatic but may have associated hydrocephalus, syringomyelia, or syringobulbia.8
Chiari I malformation is the major cause of secondary cough headache. Occipital and suboccipital pain with frontotemporal radiation in variable duration (from seconds to bouts of several weeks) and varying in quality of pain (bursting, stabbing, dull, throbbing, or lancinating) were described. Secondary cough headache began earlier in life and each attack tended to last longer than benign cough headache.7, 8
Headaches are a common presentation in patients with Chiari I malformation, although different studies show the rates vary from 15% to 75%.9 A retrospective, MRIdiagnosed Chiari I malformation case series showed fifty-nine percent of patients had or had had headaches. Fifty-two percent of Chiari I malformation patients had a headache at the time of diagnosis.8-10 The spectrum of headaches in Chiari I malformation can present as shortlasting cough headache, exertional headache, low CSF pressure headache, long-lasting headache, or continuous headache.10-13
The mechanisms of headache in Chiari I malformation have not been addressed yet. It could be two different mechanisms for short-lasting and long-lasting headaches. The mechanism of short-lasting sharp shooting headache is thought to be due to transient pressure dissociation between intracranial and intraspinal space while the patient was laughing. Differences in pressure between both compartments may cause downward displacement of the cerebellar tonsils into the foramen magnum, which causes stretching of intracranial pain sensitive structures, such as meninges, nerves, and blood vessels.8, 10, 12, 14-15 The mechanism of long-lasting dull headache has been suggested by the theory of recurrent episodes of pain originating from the craniospinal pressure dissociation that may sensitize the pontomedullary junction and the upper cervical pain pathway to produce neurogenic headache.12
Treatment of laughing headache has been reported in only one literature. Divalproex sodium was reported as an effective prophylaxis agent in laughing induced headache.4 Indomethacin was reported as a treatment in cough headache associated with Chiari I malformation.16 Decreased cerebral blood flow and reduced intracranial pressure due to vasoconstrictor effect, and/or reduced cerebral edema have been explained as the potential mechanisms of indomethacin in cough headache.17, 18
For our patient, headaches started when he was a young man of 20 years, only after vigorous laughter. Other aggravating factors did not precipitate headache. The characteristic of very short sharp shooting pain followed by long lasting dull headache on occipital area with earlier onset of symptoms suggested symptomatic cause of headache. MRI of the cervical spine found Chiari type I malformation with syringomyelia. We considered the mechanisms of laughing headache in this case could see both valve-like blockage for short-lasting headaches and sensitization of pain pathway in brainstem and upper cervical for long-lasting headaches.
Laughing headache is a rare form of triggered headache. It is mostly associated with secondary causes such as Arnold-Chiari malformation. So, we recommend an MRI for all patients who present with laughing headaches, cough headaches, patients with posterior fossa signs, or in younger patients (under the age of fifty). Unfortunately, there are no standard treatments for this condition. Divalproate sodium, indomethacine, or surgical correction of Chiari malformation should be considered as a treatment for laughing headache patient.









