Electronic ISSN 2287-0237
Several studies have been reported on spinal fracture epidemiology in specific high-energy mechanisms1-3 settings, such as motor vehicle collision, falling from a height and contact sport activities. However, spinal injuries don’t always happen on land, they also happen at sea.
On the coast, there are several water-based recreational activities that run the risk of causing spinal and other traumatic injuries.4 These include personal motorized watercraft (AKA; Jet ski, Wave-runner), speed boating, surfing, kayaking and body surfing. As these have increased in popularity in recent times, the number of accidents reported has been documented extensively in the literature. Many studies reported spinal injuries following these water-related recreational activities.5-9 However, only a small number of studies document uncommon spine injury following speedboat travel without collision and its actual mechanism of injury.10 If personal watercrafts are the motorcycles of water, then speedboats are certainly the cars. These aquatic vehicles travel at high speed across the water and their passengers are rarely wearing any protective equipment. Unfortunately, these activities have been linked to a significant risk of spinal injury when accidents occur. Each year, there is an increase in tourism to coastal regions and many tourists are less familiar with the risks and dangers associated with these aquatic vehicles. During the high season, therefore, coastal cities often experience a surge of traumatic incidents associated with aquatic recreational activities.11,12
It is commonly known that spinal injuries are most often the result of several high-energy mechanisms13-19 including motor vehicle accidents, falling from a height,20 contact sport activities and extreme sport activities.16-18 Among these spinal injuries, the thoracolumbar spine area accounted for the majority of all spinal injuries.21-23 Anatomically, this area is a transitional zone where the less mobile and rigid thoracic cages change to the more mobile lumbar spine.
Fracture classification is based on the three-column theory reported by Denis31,32 and more recently by the AO group33. This classification is essential to further understand the stability of thoracolumbar spine fractures. An unstable spine is one in which progressive anatomic deformity or neurological deficit will occur under continued stress.31,32 By definition, any fracture involving the middle column (posterior portion of the vertebral body, posterior longitudinal ligament, and the posterior annulus fibrosus) is inherently unstable.31 In a type A compression fracture, the subtypes A1 and A2 are characterized by the middle column remaining intact and acting as a hinge. The posterior vertebral body is maintained and there is no subluxation. Whilst in the other subtypes A3 and A4 injuries here involve the posterior vertebral body disruption representing a failure of the middle column which is considered an unstable spinal injury.
Thoracolumbar spine injuries are devastating injuries that can result in permanent impairment of function, when accompanied by spinal cord/nerve injury, and loss of quality of life. In some circumstances, these can be life-threatening conditions.24 To obtain an optimum outcome of treatment, health care teams should be well trained in caring for these injured patients with current spinal precaution protocols and treatments. By examining the epidemiology of injuries arising from this regional-specific setting, it is believed that more favorable treatment outcomes can be obtained through efficient safety regulations and injury management, with either non-operative or operative management.
The purpose of our study was to evaluate the epidemiology of thoracolumbar spine injuries linked to travelling by speedboat without collision at our coastal tertiary trauma center. The study aims to identify injury patterns and the mechanism of injuries to determine the link to the position seated on board with a risk of thoracolumbar injury in this type of transportation. In addition, we discuss the current safety regulations and encourage the need to improve legislation regarding marine transportation acts.
Institutional review board approval was obtained for this study. All patients were retrospectively identified from a prospectively collected database of patients admitted or treated at the emergency department, out-patient orthopedic clinic and in-patient service of the tertiary trauma center situated on Phuket, the largest island in the southern part of Thailand.
Patients enrolled from July 1, 2016 to May 31, 2018. There were 4,882 trauma patients treated or admitted during this time frame. Eligible patients were identified from ICD-10 data in the context of thoracic or lumbar spine fracture. This led to 118 patients eligible for inclusion. Traumatized patients who did not meet the inclusion criteria of having a mechanism of thoracolumbar spinal injury after travelling by speed boat were then excluded (n = 38). Finally, a total of 80 patients were included in our study. All the patients were unrestrained passengers wearing only a life jacket on board a speedboat travelling at high speed (Figure 1). They were fully evaluated with advance trauma life support and were given spinal precaution protocols initially. All of the patients sustaining thoracolumbar spine injuries underwent lateral radiographs of cervical spine, both AP and lateral radiographs of thoracolumbar spine and CT scan of whole spine to identify the morphology of spinal fracture. MRI studies were carried out when patients presented neurological deterioration or when there was a need to evaluate posterior ligamentous complex integrity.
There were a total of 80 patients in our study, 48 (60%) were men and 32 (40%) were women with a mean age of 47.50 years (Min 20, Max 71). All spinal fractures occurring in our patients are single level injuries with a total number of 80
spinal levels from 80 patients sustaining thoracolumbar spine injuries following speed boat travel (Table 1). The level of injury is located only at thoracolumbar area which involved 6 cases (7.5%) of T11 vertebra, 20 cases (25%) of T12 vertebra, 44 cases (55%) of L1 vertebra and 10 cases (12.5%) of L2 vertebra (Figure 3).Cervical or sacral region injury was not observed as well as other associated injuries such as traumatic brain injury, intra-abdominal organ injury or long bone fracture. The spinal cord/nerve root injury occurred at the thoracic region (T12) in only 1 patient (1.25%) whom presented with incomplete paraplegia.
All of the 80 patients were unrestrained on boarding. Thoracolumbar spine injuries were reported in 76 patients (95%) who sat at the front row seat and 4 patients (5%) who were in the middle seat. No thoracolumbar spinal injury was reported in our patients who sat at the rear of the boat. Patients who sat in the front row seat were significantly at higher risk for thoracolumbar spine injury (p < 0.05; odds ratio = 41.83; 95%CI: 15.24, 114.8). 50 cases (62.5%) were treated non-operatively with bracing while 30 cases (37.5) were treated operatively with computer navigation spinal surgery using pedicle screws and rods construction before being discharged or repatriated.
Table 1: Characteristic data (n = 52)
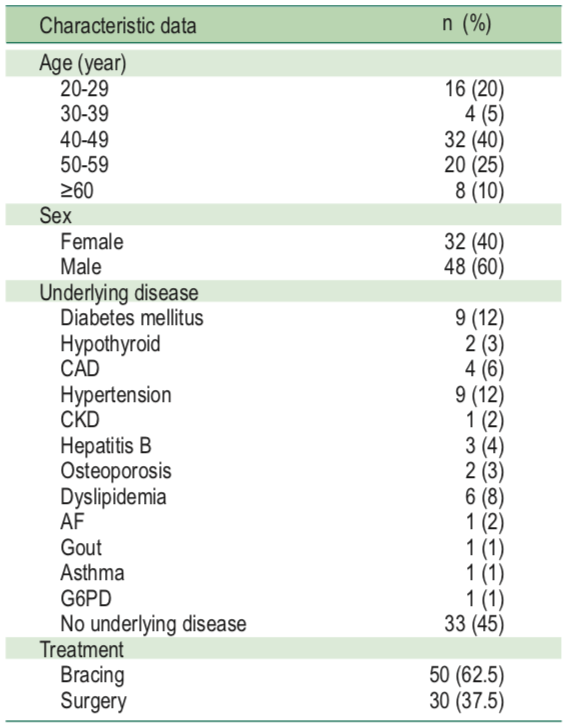

Figure 1: Speedboat (Open motor boating), the most popular transportation in coastal areas.
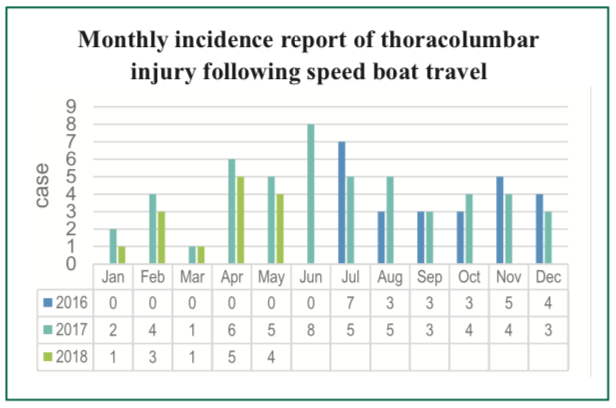
Figure 2: Monthly incidence report of thoracolumbar injury following speed boat travel.
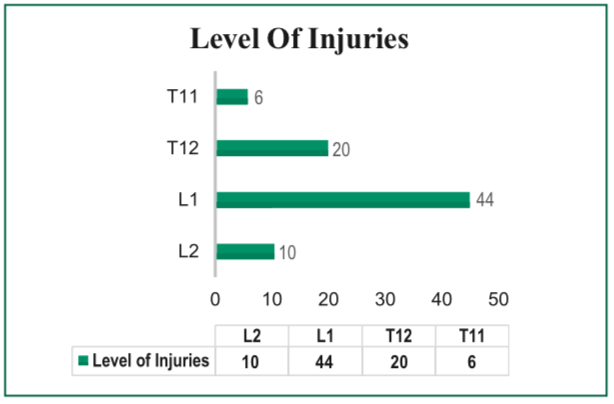
Figure 3: The most common affected vertebra following a speed boating accident is T12 vertebra followed by L1 vertebra.
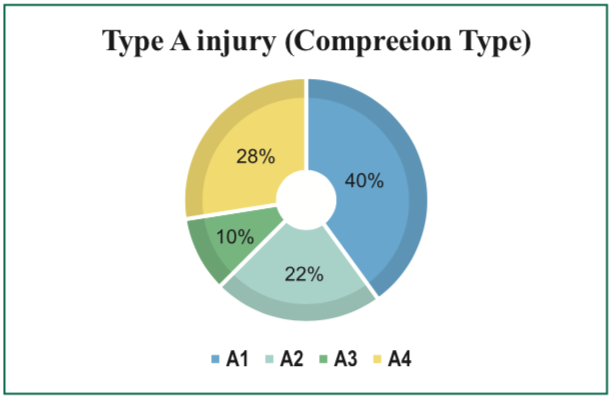
Figure 4: Classified by AO Spine TL Injury Classification, all fracture patterns in our study are type A (compression type) and divided into subtypes. A1: Compression; A2: Pincer; A3: Incomplete burst; A4: Complete burst
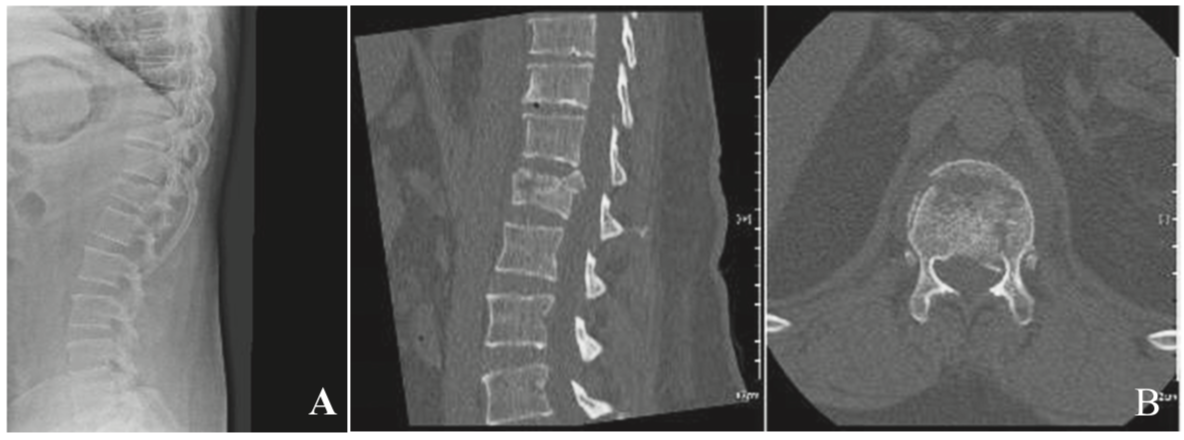
Figure 5: Imaging study of thoracolumbar spine injury after travel by speed boat.
A: Lateral radiographs of TL spine showed anterior wedge compression fracture of T12 vertebra.
B: CT scan revealed disruption of posterior vertebral body with retropulsion which is indicated.
These data indicate that spinal injuries after travelling by speedboat without collision are located mainly at the thoracolumbar junction. This transitional zone of the thoracolumbar junction accounts for the majority of thoracic and lumbar spine fractures with 90% of these injuries occurring between T11and L4 vertebrae.22,23,25 For injuries sustained on land, thoracolumbar spinal fractures are frequently common following a fall and/or high velocity automotive accidents with a higher incidence among unrestrained occupants.26-29 For injuries sustained at sea, however, the incidence of thoracolumbar spinal fractures is less common and have only been reported following diving,30 and water skiing accidents.5,6 Speedboat accidents, especially without collision, are uncommon. A review of previous literature did not reveal any documented cases of thoracolumbar spinal injuries as a result of speed boating without collision. To our knowledge, this is the first large-scale reported case series of its kind.
The fracture morphology presented in our study is only type A (compression type) classified by AO classification. Although, compression injuries are the most common injury to the thoracolumbar spine, representing 48% of all thoracolumbar spine fractures and 58% of all major spinal injuries,31,32 tension band and displacement/translation injuries have also been observed in several high-energy mechanism of injury. It is very interesting that there was no tension band injury or displacement/ translation injury observed in our study. The fracture morphology confirmed by CT scans represent only the compression type of fracture which indicates that compression injury is a unique characteristic of thoracolumbar fracture after travelling by speed boat.
Thoracolumbar spinal fractures following road traffic accidents are mostly flexion injuries.34 Thoracic spine injury in the unrestrained motorcyclist is thought to occur as the result of hyper-flexion of the spine on impact with objects,35 with maximal loading and injury at the level of the mid thoracic vertebrae (T4-T7).27,36 The higher incidence of low levels of thoracic spinal injury in car occupants may reflect protection of the thoracolumbar spine afforded by the seat and seat belt.37
In our series, patients report the mechanism of the injury involved in an event including flexion of their spine during the boat’s climbing on to the wave followed by a sudden deceleration of the boat when landing back on to the water surface which resulted in sudden flexion and an axial compression loading of their thoracolumbar spine. This mechanism was observed in all of the reported cases, resulting in compression type injuries, based on the Allen-Ferguson classification,38 at different levels of the thoracolumbar spine of the unrestrained speedboat passengers.
More importantly, our case series show a link between the position on board where a person is seated and the risk of thoracolumbar spine injury. Patients who sat at the front were at highest risk for sustaining thoracolumbar spine injury. This can be envisaged as the speedboats place their engine at the rear, resulting in an elevation of the front part of the boat, which is at least 1-1.5 meter higher than the water surface. When the boat encounters a big wave at high speed, the boat is suddenly halted, climbing up the wave and landing back forcefully on the water’s surface. This resembles the actual mechanism of a fall from a height that causes a sudden forward flexion and axial compressive load to the thoracolumbar spine area. Furthermore, the center of gravity of the human body is in front of thoracolumbar area causing the anterior and middle column of thoracolumbar spine to always be under a compressive force while the posterior column is under a tensile force. All of these conditions support the unique injury findings that all the thoracolumbar fractures that occurred in our case series are of a compressive nature.
A limitation of this study was the retrospective nature of the analysis that may be more susceptible to selection bias. Although all data were collected prospectively, it was not recorded with the current study in mind and it is possible that some pertinent data may have been overlooked. In fact, each boat’s occupancy rate might slightly differ from what we calculated by using a 100% occupancy rate and this might result in a change of statistical significance of disease/injury links.
We found a high incidence of thoracolumbar spine injuries linked to speed boating without collision. Most injuries were compression fractures between T11-L2. The majority of patients reported being seated on the front row seat of the speed boats. As a result, practitioners who are responsible for trauma patients in coastal areas should be made aware of the significantly increased risk for injuries linked to being seated at the front of the speed boat. Proper spinal injury precautions must be universally complied with to optimize treatment outcomes. Current safety regulations, in particular speed limits, proper safety restraint techniques, bracing position on board and protocols for marine rescuers should be carefully reviewed. These improvements would lead optimistically to greatly reducing the number of victims and the extent of the degree of injuries experienced currently.
None declared.









