Electronic ISSN 2287-0237
High sodium is a major risk of hypertention and cadiovascular dieases worldwide, leading to disability, decreased quality of loife and premature deaths.1 Thailand is an Asian country with high sodium intake in its population, consistent with Japanese, and Chinese with approximately twice of the recommended intake, at 2,000 mg/day.2-5
The World Health Organization set the goal to reduce sodium intake by 30% by 2025.6 All sectors were encouraged to take part to reduce causes of the diseases by emphasizing appropriate food consumption behavior. Education institution has also realized the significance of sodium intake reduction among its faculty members, staffs, as well as students living in on-campus dormitories.
Nursing students are in the transition period from adolescence to adulthood. Their food consumption behaviors are influenced not only by intrapersonal and interpersonal factors, but also physical, and social environment, particularly foods available on campus and promoted by the media. The average sodium consumption in Thai adolescents aged 16-18 years was 3,536.9-4,602.7 mg/day.7 In addition, the majority of the nursing students (85.8%) had limited knowledge on which food contains sodium, including bread and bakery products and thought that these products contained no sodium.8 Therefore, they are considered a target for health promotion aimed to reduce sodium intake through behavioral modification and to develop healthy food habits, ensuring that they are role models in nursing.
A systematic review and meta-analysis revealed that sodium intake was positively associated with blood pressure in adolescents.9 To primarily prevent hypertension, health promotion strategies should be implemented through education intervention aimed at limiting sodium intake.10 Previous studies focused on various populations in- cluding nursing students; however, it was a preliminary study conducted in only one setting.11-14 Thus, this study aimed to investigate effects of the program promoting food consumption for sodium reduction on knowledge of sodium consumption and urinary sodium in nursing students.
Hypothesis
It was hypothesized that after the program, knowledge on sodium consumption in nursing students is higher than the baseline and before the program. Urinary sodium is lower than the baseline and before the program and score of sodium consumption behavior after the program is lower than the baseline.
This study used a quasi-experimental design with a one group self-control design. Through convenience sampling with inclusion criteria, the participants consisted of 173 second-year undergraduate nursing students in three nursing schools: two in Bangkok, the capital city (n = 117), and one in a province of the western region (n = 56) between April and May 2016. The inclusion criteria were:
Sample size was determined according to Stevens15 using the effect size 0.14 from the previous study16, power of the test 0.80, and the level of significance of 0.05, obtaining sample size of 165. An additional 5% was added to allow for participants dropping out of the study, resulting in the final sample size of 173.
Instruments
The knowledge of sodium consumption questionnaire
was a self-reported questionnaire modified with permission from the previous study8, consisting of 16 items that asked about their knowledge on the following subject : sodium, nutrition label, consumption of food containing high sodium, hidden sodium content, and the effects on health. The response item included ‘yes,’ ‘no,’ and ‘not sure.’ The correct answer was scored as 1 while the incorrect answer or not sure was scored as 0. Interpretation was classified into 3 levels: good (> 80%), moderate (50-79.9%), and poor (< 50%). Reliability of the original version of knowledge of sodium consumption questionnaire, Kuder-Richardson (KR-20) was 0.82. In the present study, KR-20 was 0.79.
The sodium consumption behavior questionnaire was modified with permission from Piaseu et al.,8 consisting of 13 items with three subscales including use of nutrition label, consumption of food containing sodium, and use of seasonings. The response item was 5-point Likert scale ranging from 1 (never) to regularly (5). Interpretation was classified into 3 levels based on percentage: good (> 80%), moderate (50-79.9%), and poor (< 50%). Test-retest reliability of the original version of the questionnaire was .89 and the present study was 0.78.
Urine collection was completed twice for a period of 12 hours, from 7 pm to 7 am, on three occasions at four-week intervals. At the dormitories, urine was collected in labeled containers after instructions had been provided. The 24-hour urinary sodium was then determined in the laboratory for the average at baseline, before and after the program.17,18
Intervention
The program promoting food consumption for sodium reduction was developed according to health promotion strategies including the SHAKE Technical Package for Salt Reduction (Surveillance: measure and monitor salt use, Harness industry: promote reformulation of foods and meals to contain less salt, Knowledge: educate and communicate to empower individuals to eat less salt, and Environment: support setting to promote healthy eating19). This was integrated with four processes that promote sodium reduction: Raising awareness, Aiming at target outcome, Mobilizing change and innovation, and Assuring synergy20 (Table 1).
The program, examined for content validity by three experts, consisted of manuals developed by the Potential Development of Thai People Project:
measure sodium content in liquid cooked foods. The yellow color indicated a low level of sodium, ranging from 0.4-0.7% while the green color indicated a reasonable level of sodium, ranging from 0.8-1.1% and the red color indicated a high level of sodium, ranging from 1.2-1.4%.
Data collection
After written consent was provided, demographic data and health assessment of each participant was collected at baseline including age, gender, body mass index (BMI), blood pressure, and health problems. The participants were assessed for knowledge on sodium consumption and 24-hour urinary sodium at baseline (week 0), week 4, week 8, and received explanation on how to record each meal onto the food consumption record form. During the control period, they were informed to carry out their activities as usual. The program promoting food consumption for sodium reduction was implemented during week 4 and 7 in each institution. The program was conducted with an emphasis on participation in group processes focusing on four activities as described in Table 1.
Table 1: Program promoting food consumption for sodium reduction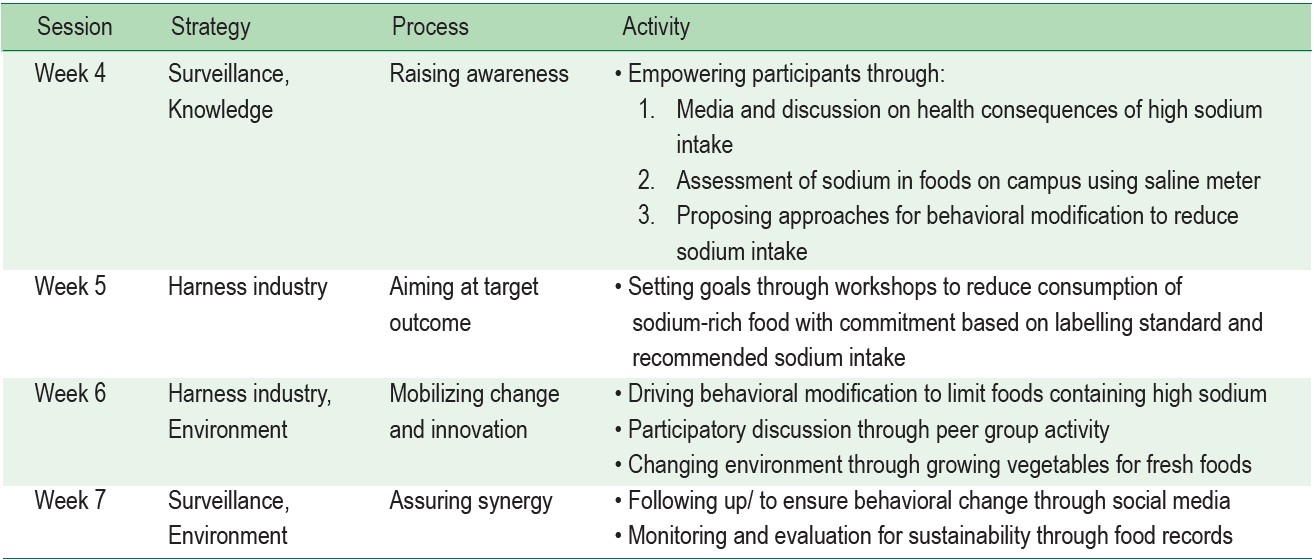
After raising awareness, participatory goal setting was conducted through workshops at which participants were asked to analyze obstacles to reduce sodium intake. They then established a mutual agreement to mobilize behavioral changes including:
The participants also learned how to calculate their daily sodium intake from the manuals on nutritional labels of seasonings and processed foods, and discussed with their peers. Food records were completed for monitoring and following up to ensure behavioral change along with use of social media.
Ethical consideration
This study was approved by the Ethical Committee, Faculty of Medicine Ramathibodi Hospital, Mahidol University (No.2559/31: 01-59-31). The participants were approached and informed of study details before informed consent was obtained with a right to withdraw from the study at any time.Data were kept confidentially.
Data analysis
Descriptive statistics were used for demographic data. One-way Repeated Measures ANOVA was used to compare urinary sodium and knowledge while Paired t-test was used to compare sodium consumption behavior at baseline and after the program. Bonferroni was used for multiple comparison.
There was no dropping out over the period of the study. Majority of participants were female (92.5%) with a mean age of 19.6 ± 0.6 years, with a normal body mass index (55.5%). Approximately 10.4% of the participants were overweight (BMI 23-24.9 kg/m2), while 24.9% were underweight (BMI < 18.5 kg/m2). Their mean systolic blood pressure was 104.1±10.8 mmHg, and diastolic blood pressure was 67.4 ± 7.9 mmHg.
Overall knowledge on sodium consumption and subscales on consequence of high sodium intake, and nutrition label were moderate, while food containing sodium was good, and hidden sodium content was poor. One-way Repeated Measure ANOVA and multiple comparison revealed that after the program, knowledge was higher than before the program and the baseline (p < 0.001) while no difference was found between baseline and before the program (Table 2, 3, 4).
The overall sodium consumption behavior and subscales, including use of nutrition label, consumption of food containing sodium, and use of seasonings were moderate. Paired t-test revealed that after the program, mean score of sodium consumption behavior was lower than baseline (Table 2, 5).
Urinary sodium was 1,685.3 ± 800.3 mg/day on average. One-way Repeated Measure ANOVA and multiple comparison revealed that after the program, urinary sodium was lower than before the program and the baseline (p < 0.001) while the urinary sodium before the program was higher than the baseline (p < 0.001) (Table 2, 3, 4).
Table 2 : Baseline knowledge, behaviors, and urinary sodium of the participants (n = 173)
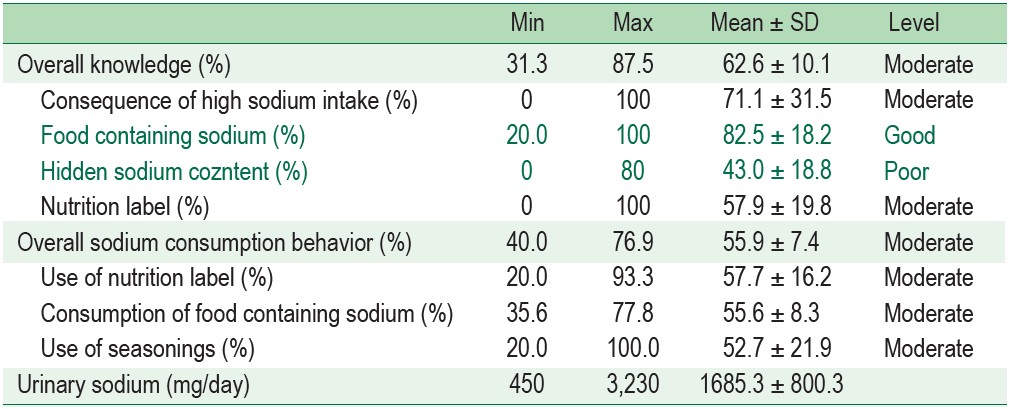
Table 3 : Comparison of knowledge, and urinary sodium in participants at baseline, before program, and after program using One Way Repeated measures ANOVA (n = 173)
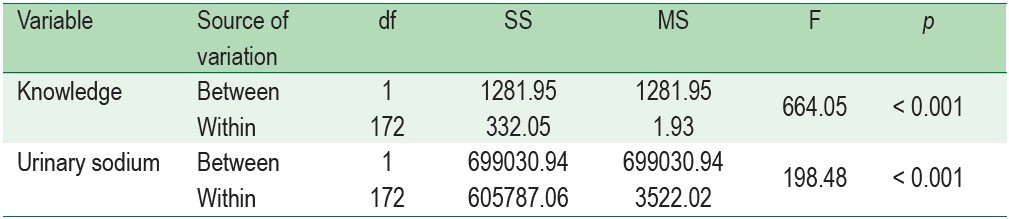
Table 4 : Comparison of knowledge, and urinary sodium in participants at baseline, before program, and after program using One Way Repeated measures ANOVA (n = 173)
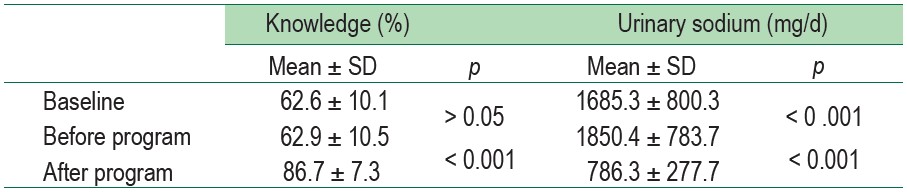
Table 5 : Comparison of sodium consumption behaviors in participants at baseline and after the program using Paired t-test (n = 173)
At baseline, the participants had a moderate level of knowledge and sodium consumption behavior, consistent with their urinary sodium. The average of urinary sodium in this study was lower than the most recent national survey.7 This may be partly due to a response to sodium reduction policy.
The results showed that knowledge on sodium consumption was not changed in the control period while it increased in the intervention period. Also, the score of sodium consumption behavior was significantly lower after the program than the baseline. Moreover, the urinary sodium increased in the control period but decreased in the intervention period, indicating that the program promoting food consumption for sodium reduction enabled the participants to increase their knowledge and reduce sodium consumption behavior, resulting in decreased urinary sodium.
The program raised participants’ awareness of problems caused by the consumption of food high in sodium through use of the saline meter in various foods on campus which could help them become aware of selecting food with low sodium in everyday situations. In addition, the participants set a goal to reduce sodium and mobilize behavioral modification in their peer groups that were considered a social and environmental factor facilitating behavioral modification, resulting in better sodium consumption behavior. Although adolescents generally tend to prefer a single ready-to-eat dish, which results in sodium consumption that exceeds the recommendation,24 the goal to drive behavioral modification was set and theparticipants were informed that consumption of food containing low sodium could help prevent hypertension.
Results in this study indicated that the program promoting food consumption for sodium reduction was sufficient to reduce sodium consumption behaviors and urinary sodium in the participants. The results were consistent with previous studies that used participatory process, medias, and groupsupport for behavioral modification.25-27
A one-group quasi-experimental design with self-control was used in this study. The findings may have resulted from testing effect for the knowledge test. However, this design helped reduce errors that may have been caused by individual differences.
Based on the study results, it is recommended that health teams apply the program including raising awareness, aiming at target outcome, mobilizing changes and innovation, and assuring synergy as appropriate to promote food consumption for sodium reduction among nursing students and extend to other populations
After the program, knowledge was significantly higher while urinary sodium was lower than before the program and baseline. Sodium consumption behaviors were lower after the program than baseline.
The authors are thankful to all participants in this study, Ramathibodi School of Nursing, Faculty of Medicine Ramathibodi Hospital, Mahidol University and the Global Network for Health for research funding.









