Electronic ISSN 2287-0237
To evaluate the diagnostic accuracy of 256-slice Multidetector Computerized Tomography (256-MDCT) in detection of coronary graft patency by comparison with the gold standard invasive coronary angiography (ICA).
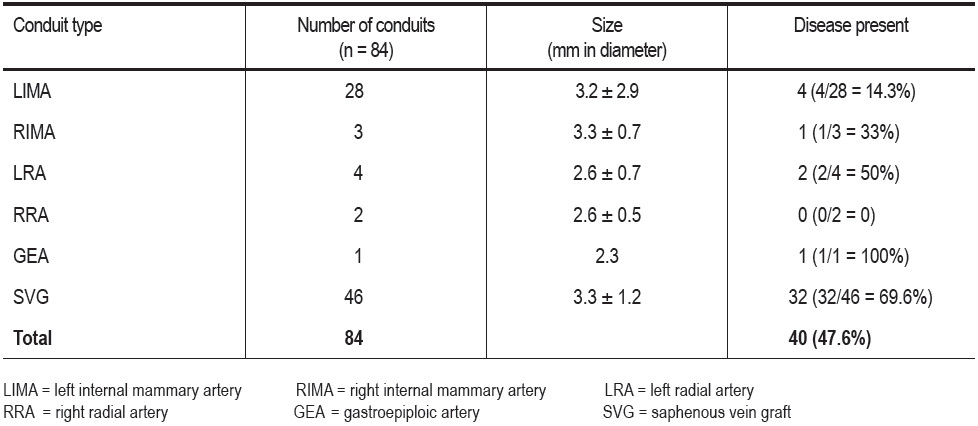
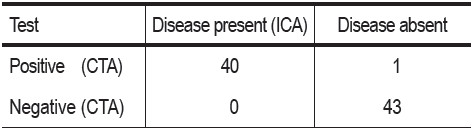
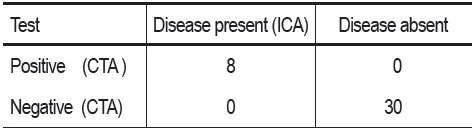
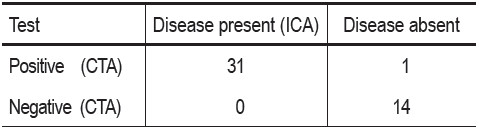
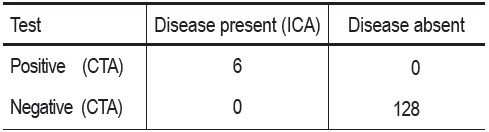
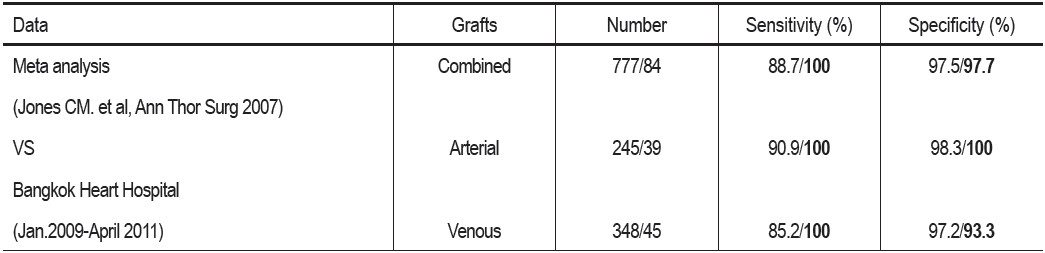
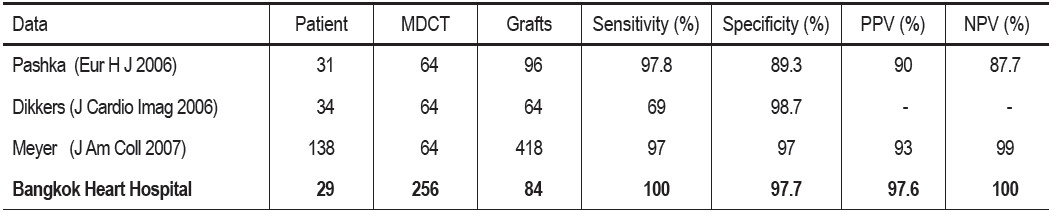
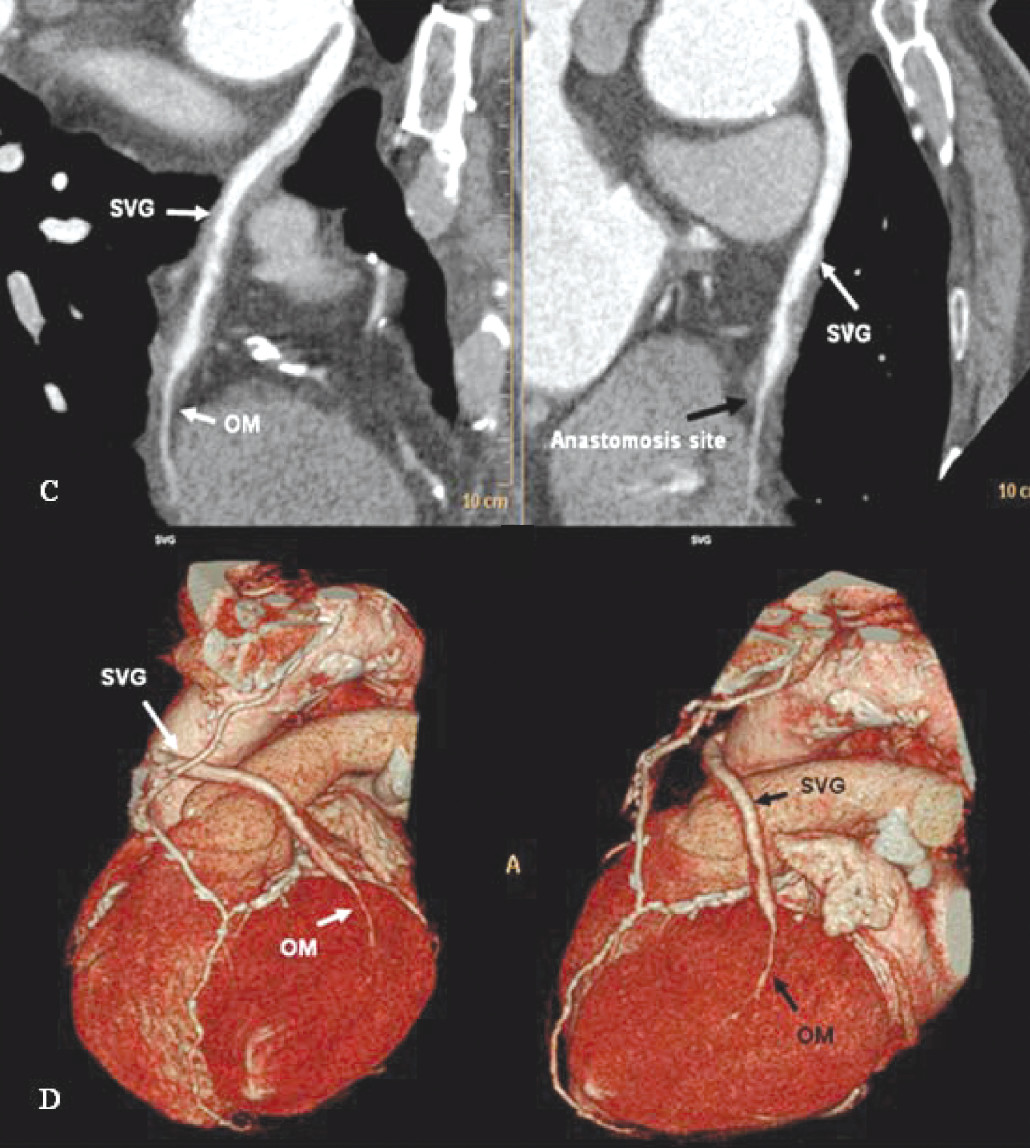
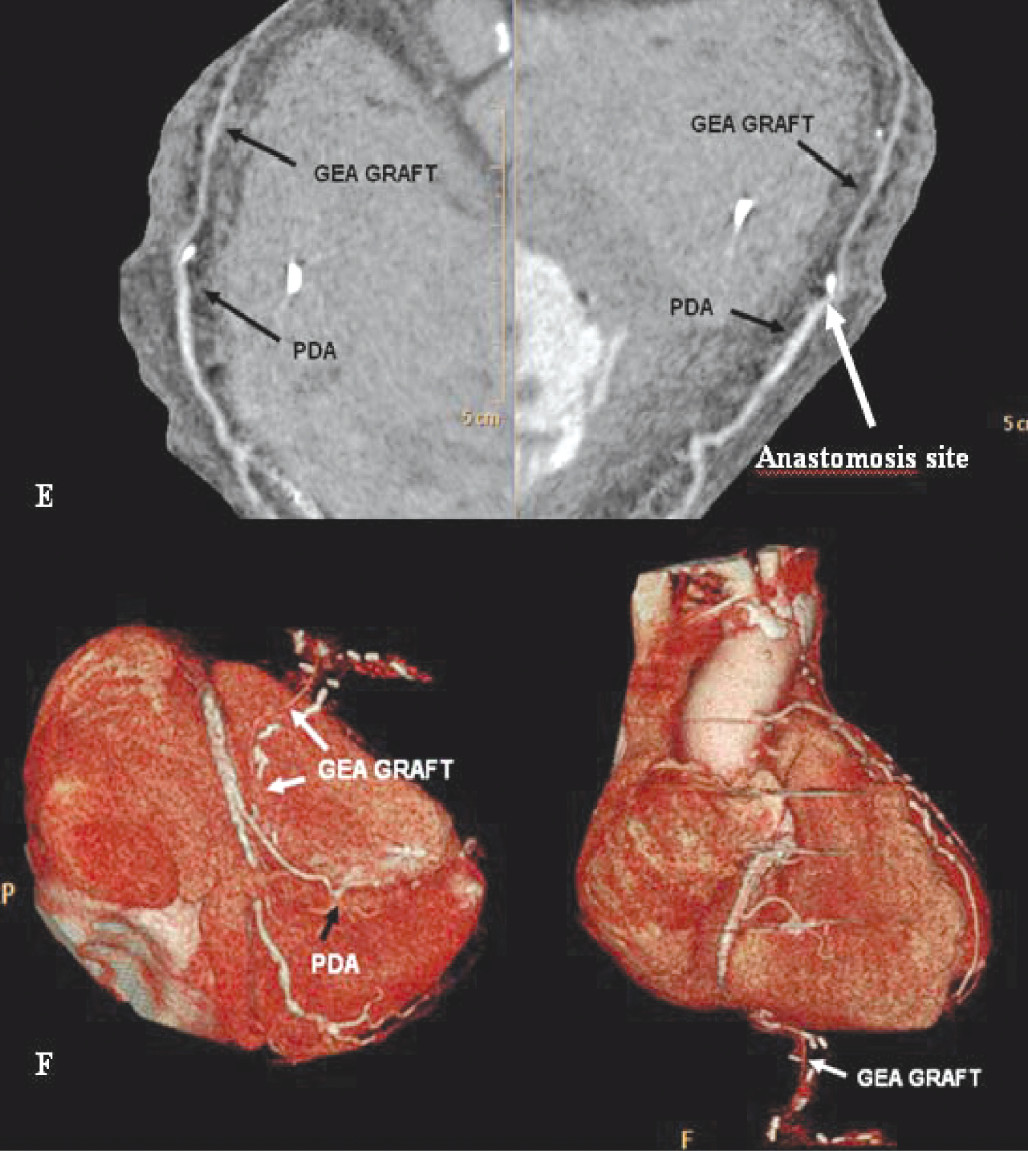
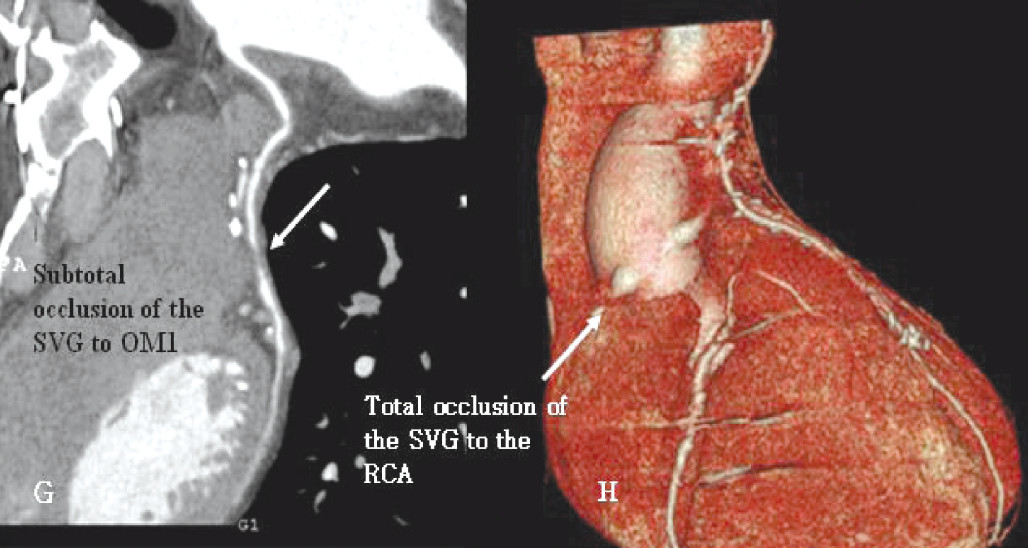
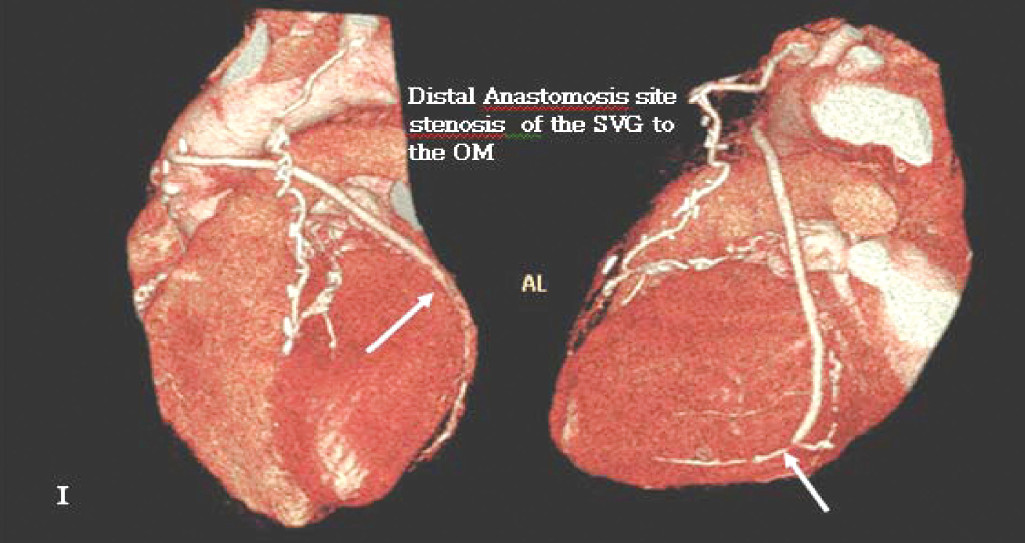
From January 2009 to April 2011, a total of 29 consecutive patients who had previously had CABG surgery were referred to us for assessment of graft patency. A total of 84 coronary bypass graft conduits (38 arterial graft conduits, 46 venous graft conduits) were studied, using 256-MDCT and ICA with iodine contrast intravenous injection. All patients underwent coronary angiography to either confirm result or PCI of graft disease. The diagnostic accuracy of the 256-MDCT for coronary bypass graft evaluation was assessed by comparing it to the ICA in terms of sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV).
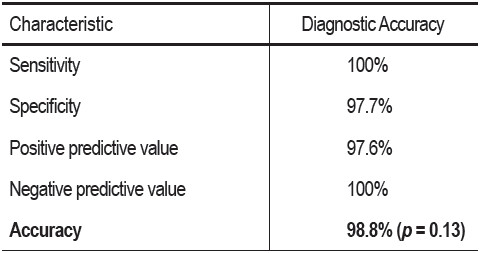
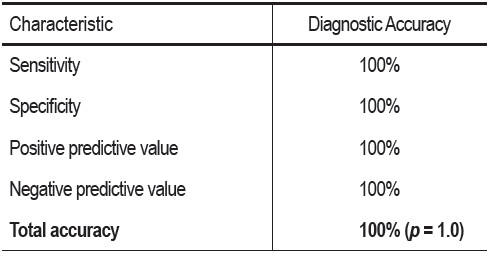
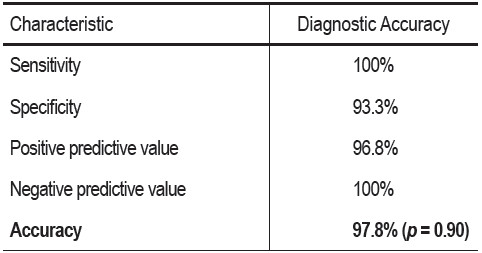
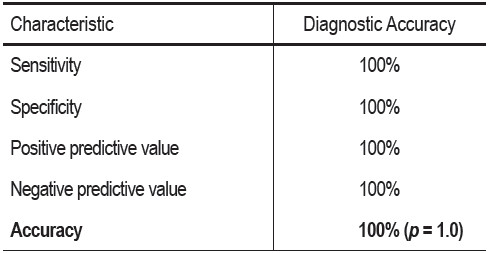
A total of 84 grafts were imaged using the 256-MDCT and all grafts were visualized. There was no statistical difference in diagnostic accuracy between MDCT and ICA regardless of the age, size or type of the bypass graft conduit (p value = 0.13). The sensitivity, specificity, positive predictive value, negative predictive value of 256-MDCT in coronary artery bypass graft assessment were 100%, 97.8% , 97.5% and 100 % respectively.
The 256-MDCT provides a high accuracy, reliability and feasibility for coronary bypass graft evaluation and the diagnostic accuracy is comparable to the gold standard ICA.
Coronary bypass graft, 256-MDCT, Invasive coronary angiography, Sensitivity, Specificity, Positive predictive value, Negative predictive value, Accuracy
10.31524/bkkmedj.2011.09.002