Electronic ISSN 2287-0237
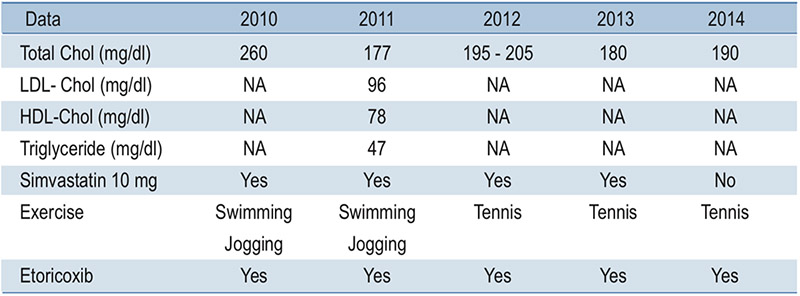
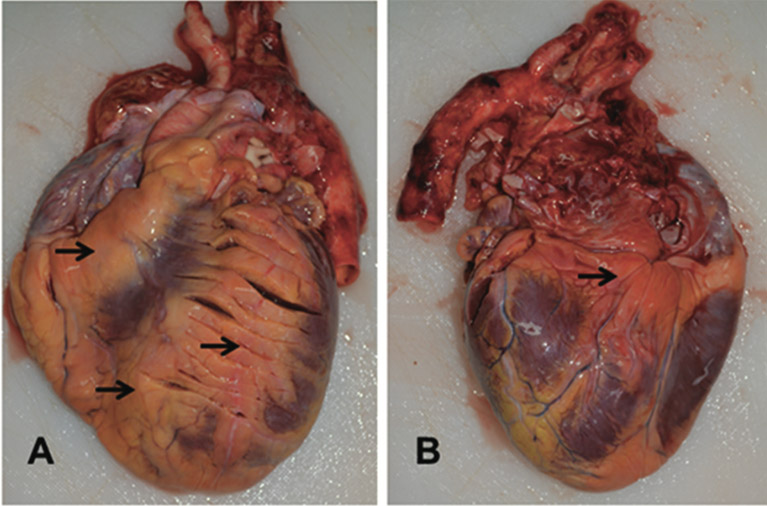
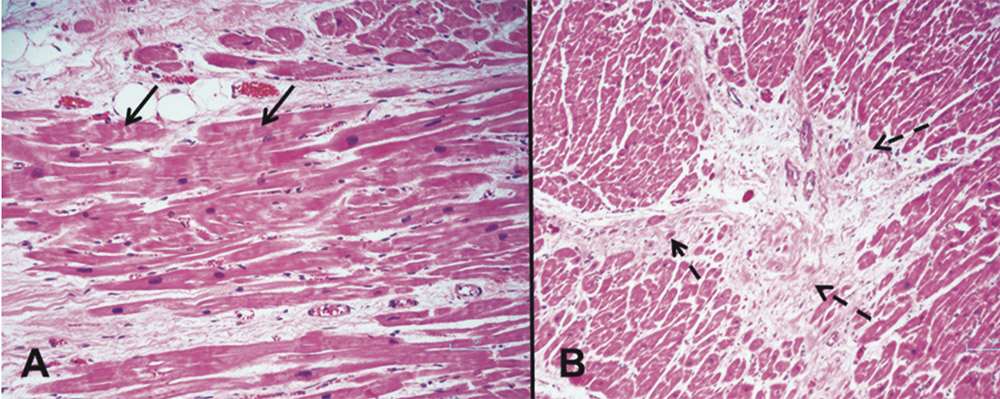
Acute Myocardial infarction (AMI) at a young age (below 45 years) is rare anddifficult to predict. We reported a fatal myocardial infarction from advanced atherosclerosisin a healthy young man who had no other major coronary risk factors except mildhypercholesterolemia. Thus, all available systemic risk scores identified him as a low riskcandidate for developing a cardiovascular event. Autopsy revealed advanced atherosclerosisin all three major coronary arteries causing acute and old myocardial infarction. Thickepicardial adipose tissue and myocardial bridging of the mid left anterior descendingartery were also noted. He frequently used etoricoxib to treat knee and back pain forconsecutive five years. Potential mechanisms of sudden death from atherosclerosis, myocardialbridging, epicardial adipose tissue and selective COXIB are discussed in moredetail below.
sudden death, young myocardial infarction, premature atherosclerosis, mild hypercholesterolemia, myocardial bridging, epicardial adipose tissue, COX 2 inhibitor
Received: January 28, 2019
Revision received: January 28, 2019
Accepted after revision: January 31, 2019
BKK Med J 2019;15(1): 66-72.
DOI: 10.31524/bkkmedj.2019.02.012