Electronic ISSN 2287-0237
To report functional and radiological outcomes of open reduction and internal fixation of proximal humeral fracture with anatomical LCP using 6 stepwise intraoperative criteria in surgical procedures.
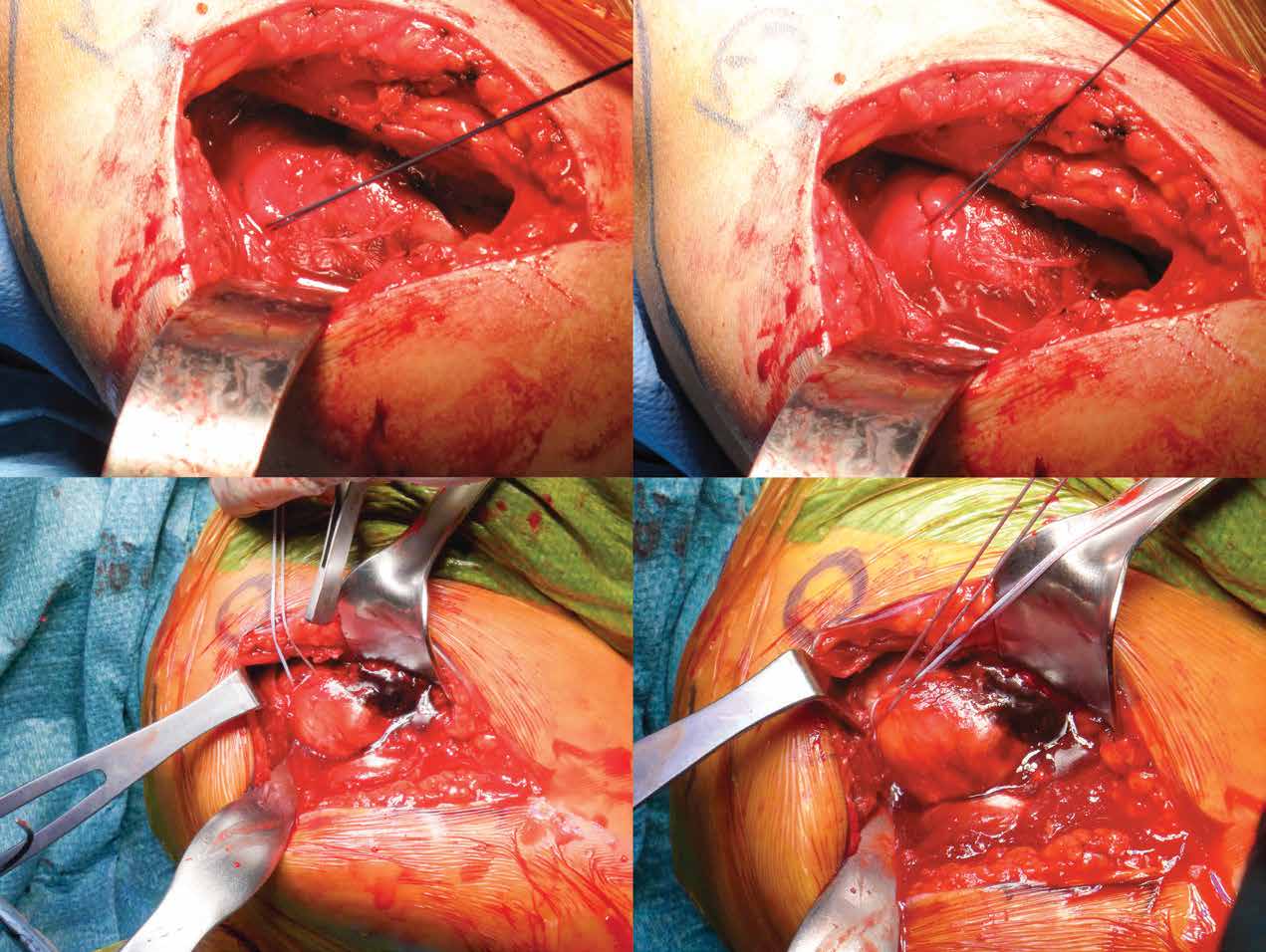
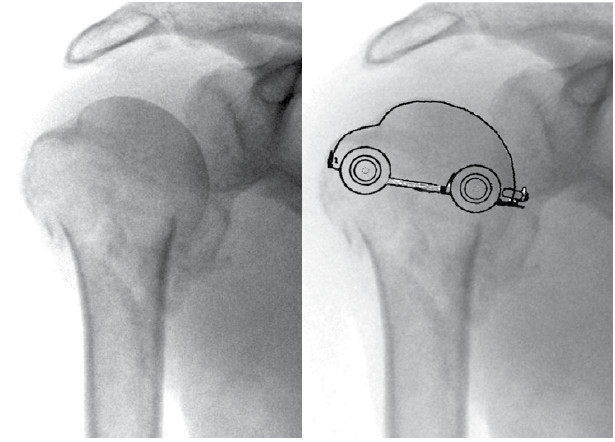
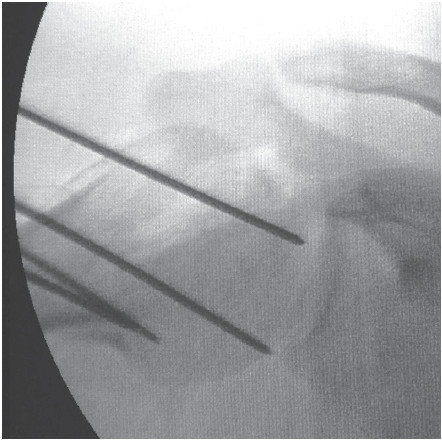
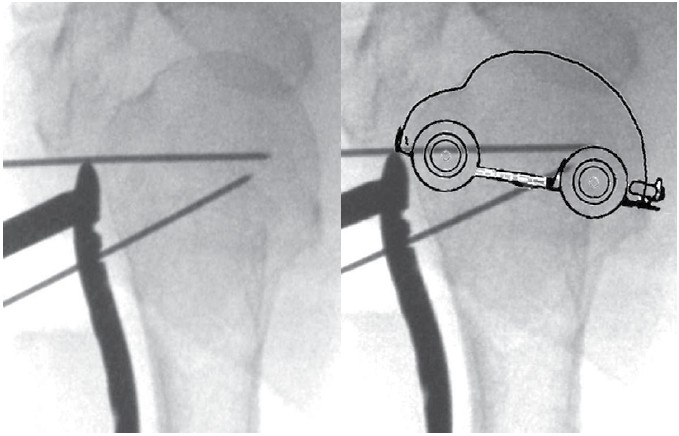
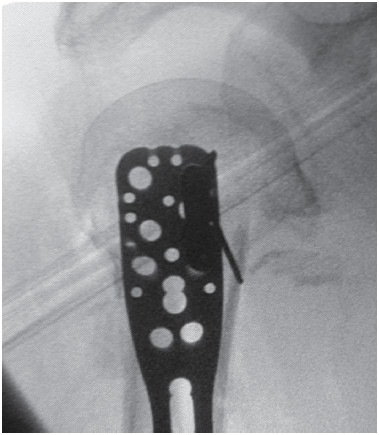
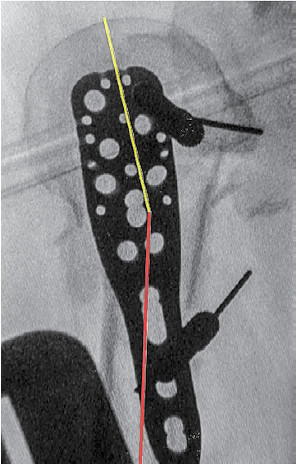
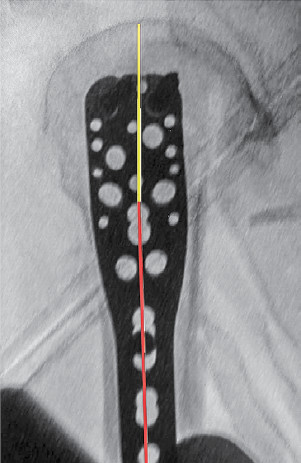
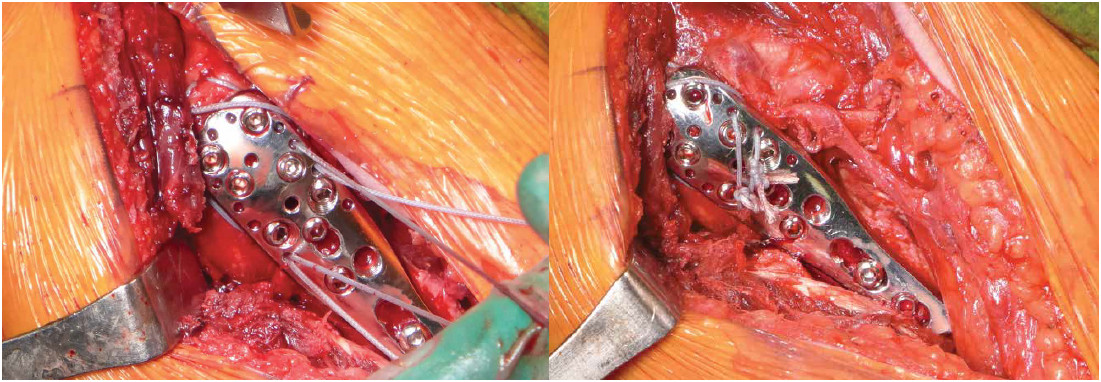
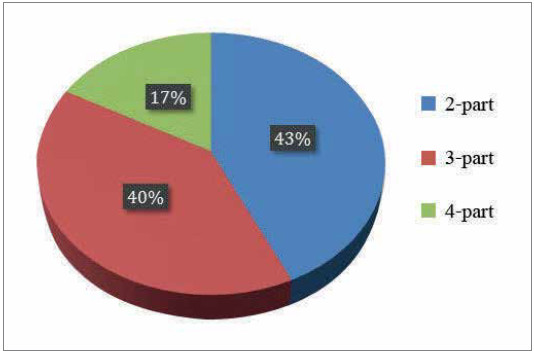
A total of 30 proximal humeral fractures which were treated with open reduction and internal fixation with anatomical LCP of proximal humerus at a Level 1 and a Level 2 trauma center between January 2012 to December 2015 were collected. All patients were operated using the same technique in the supine position on a radiolucent table. The surgical approach was delto- pectoral approach. The operation was strictly done following 6 stepwise intraoperative procedures, this included: Step 1) reduction and fixation of head fragments. The reference image in the true AP fluoroscopic view named “beetle car” appearance was applied in all cases; Step 2) plate positioning with the humeral head, according to recommendation of implant surgical instructions; Step 3) fix the plate to the humeral head; Step 4) plate positioning to the shaft; Step 5) fix the shaft to the plate including additional locking head screws, head and calcar fixation and; Step 6) secure the sutures of the cuff to the plate. All patients received a similar physical therapy program following internal fixation. According to the Neer’s classification, there were 13 two-part fractures, 12 three-part fractures and 5 four-part fractures. The functional outcomes, Constant scores, and radiological outcomes (head-shaft angle and complications) were analyzed. The mean follow-up time was 18 months.
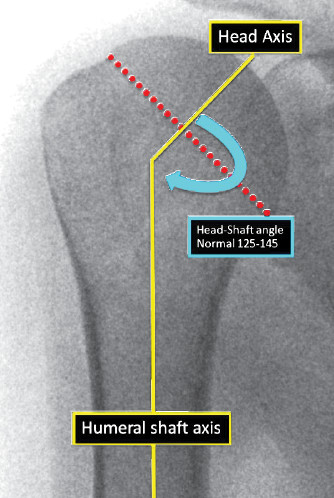
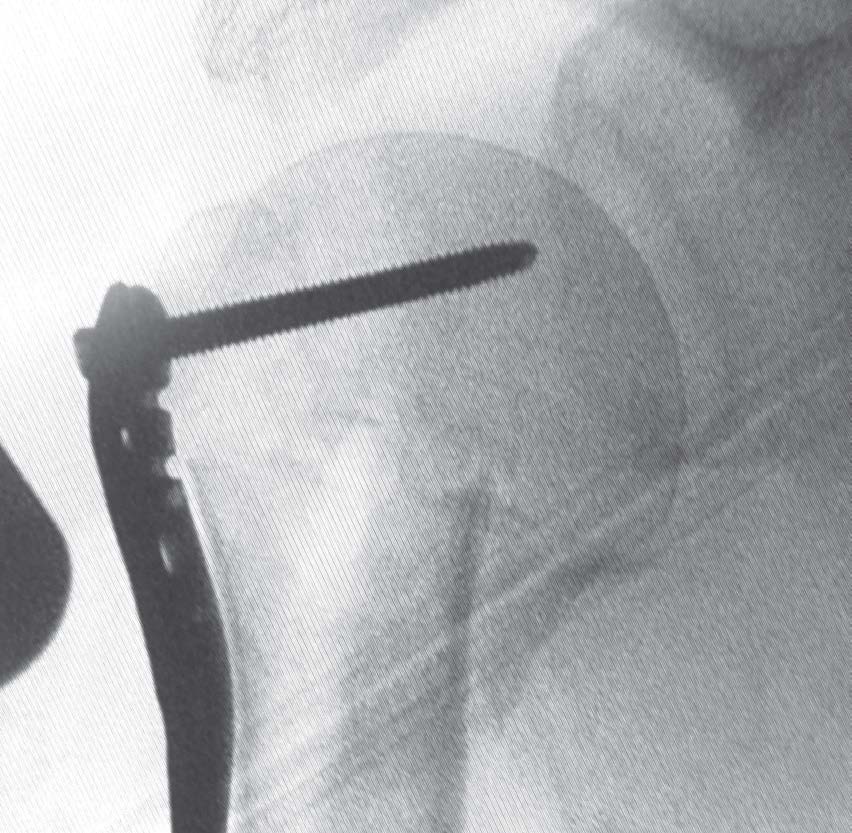
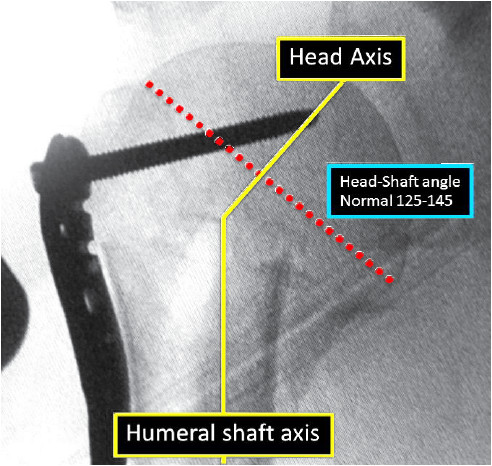
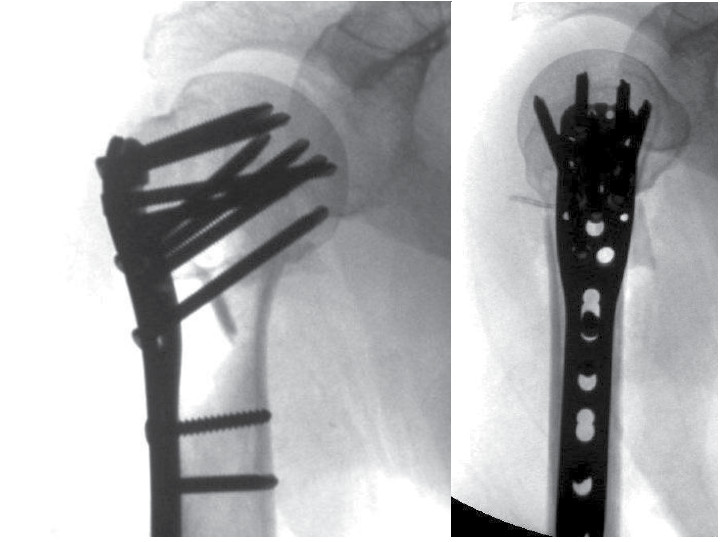
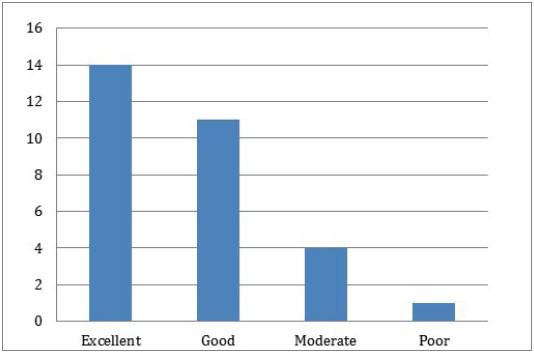
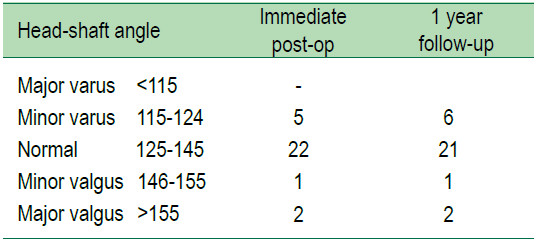
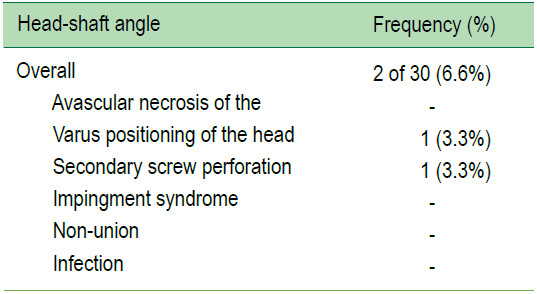
At the end of the follow-up period, all fractures united with acceptable alignment. The mean Constant score for the injured side was 86 points (range 42–92). Head-shaft angle minor varus (115-124) in 5 patients, normal (125-145) 22, minor valgus (146-155) 1 and major valgus (>155) in 2 patients. 2 patients (6.6 %) had complications which was confirmed by radiologic assessment. It was also found that one case had secondary intraarticular screw penetration and another had secondary varus during follow up. Both of the cases had severe osteoporosis, but no reoperation was required.
This study reports on the functional and radiological outcomes of open reduction and fixation of displaced proximal humeral fracture with anatomical locking compression plate using these developed 6 stepwise operative procedures which showed reasonable good to excellent outcomes with low complications. This study strongly suggested that the 6 stepwise surgical procedures should be strictly followed in the correct order as a surgical strategy to prevent complications arising from the operative technique of internal fixation of the complex proximal humeral fracture. from the operative technique of internal fixation of the difficult proximal humeral fracture.
proximal humeral fracture fixation, true AP view, beetle car appear- ance, true lateral view of plate, secondary varus, screw penetration
10.31524/bkkmedj.2016.09.001