Electronic ISSN 2287-0237
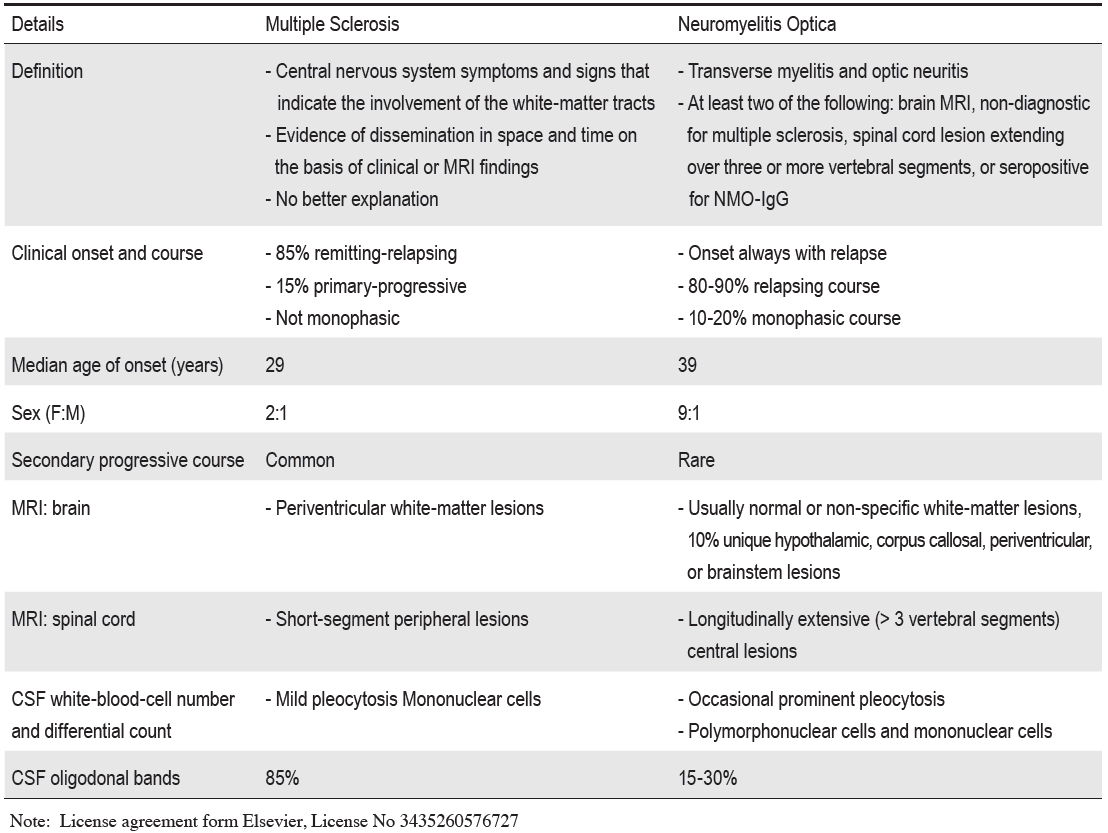
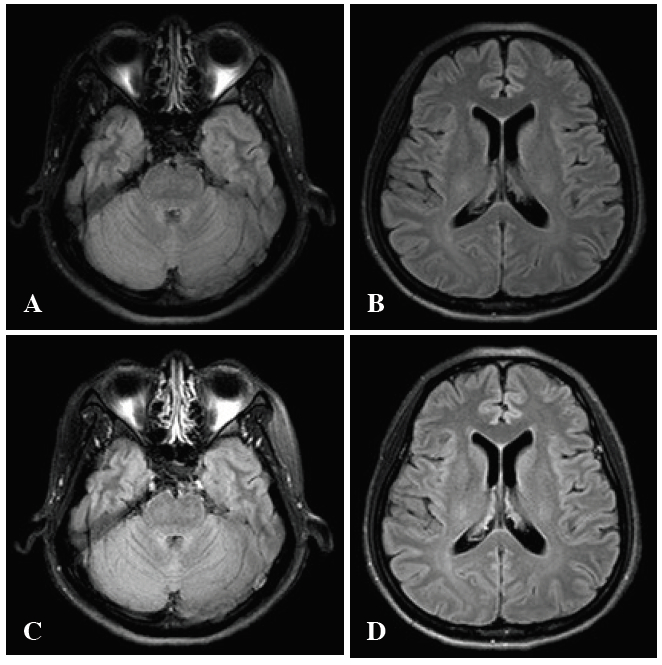
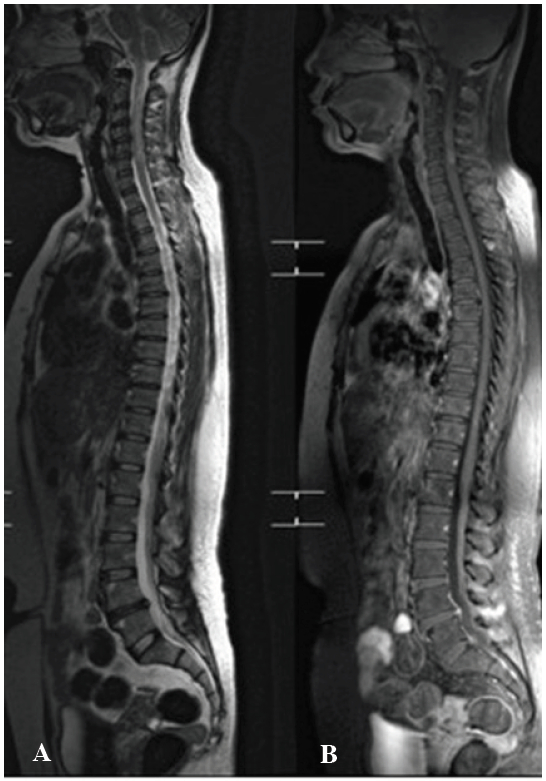
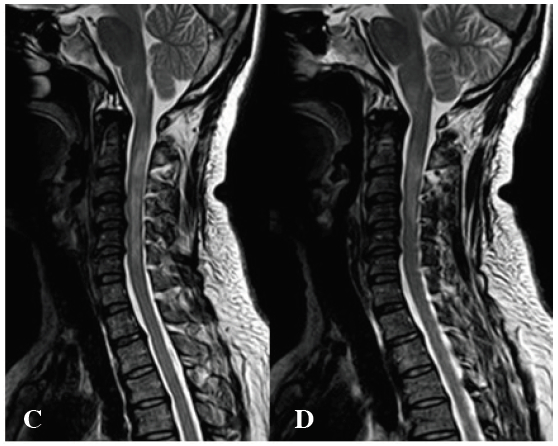
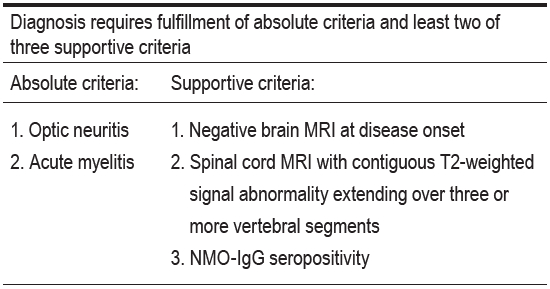
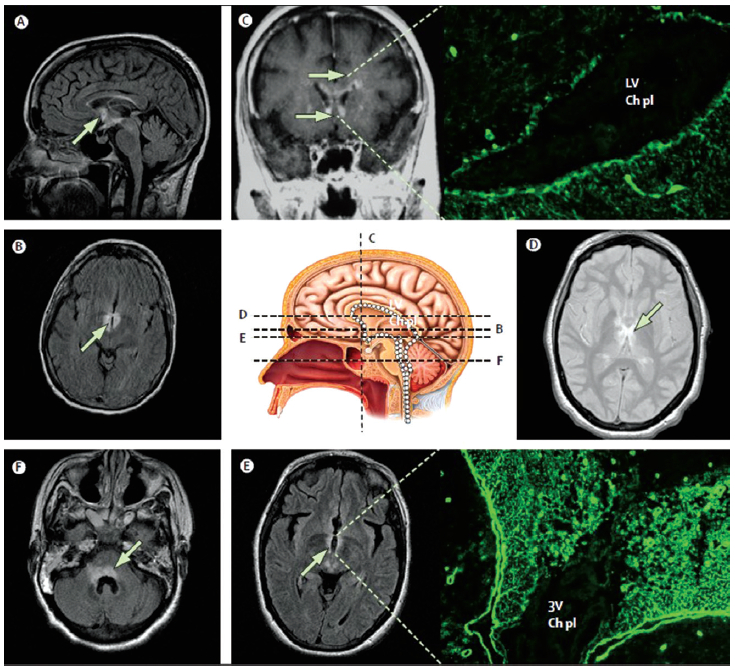
NMO is a is a rare entity which involves the central nervous system acting as an inflammatory process by attacking the optic nerve (ON) and longitudinally extensive transverse myelitis (LETM). The specificity of this disease is antibody aquaporin-4 (AQP4). Repeated relapses of the disease can lead to severe disability and blindness. MRI is none specific but at the cervical spinal cord shows the long extensive contrast enhancement. The specific diagnosis is NMO IgG.
neuromyelitis optica, NMO-IgG, aquaporin-4 antibody, APQ-4, multiple sclerosis, MS, oligoclonal band, azatrioprine
10.31524/bkkmedj.2014.09.007