Electronic ISSN 2287-0237
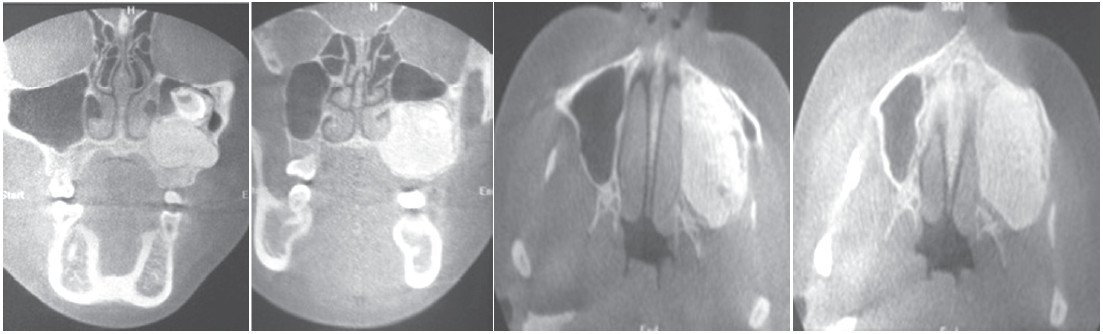
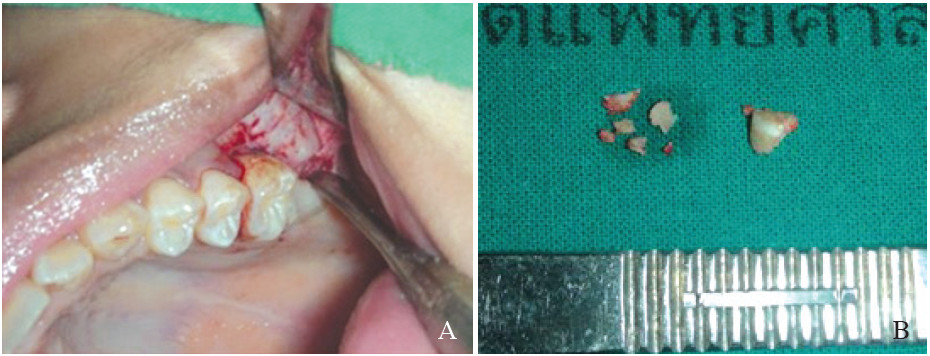
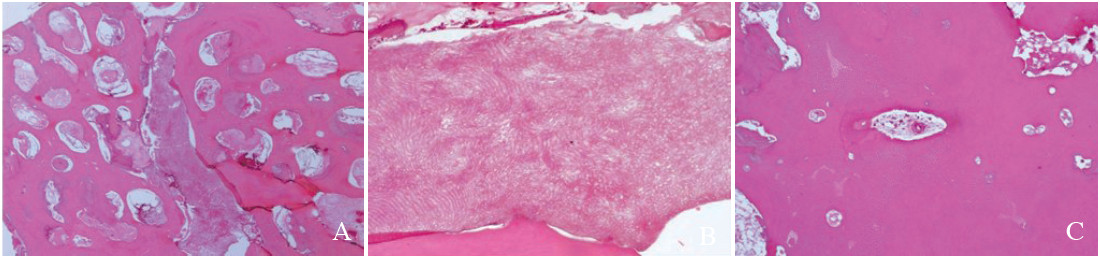
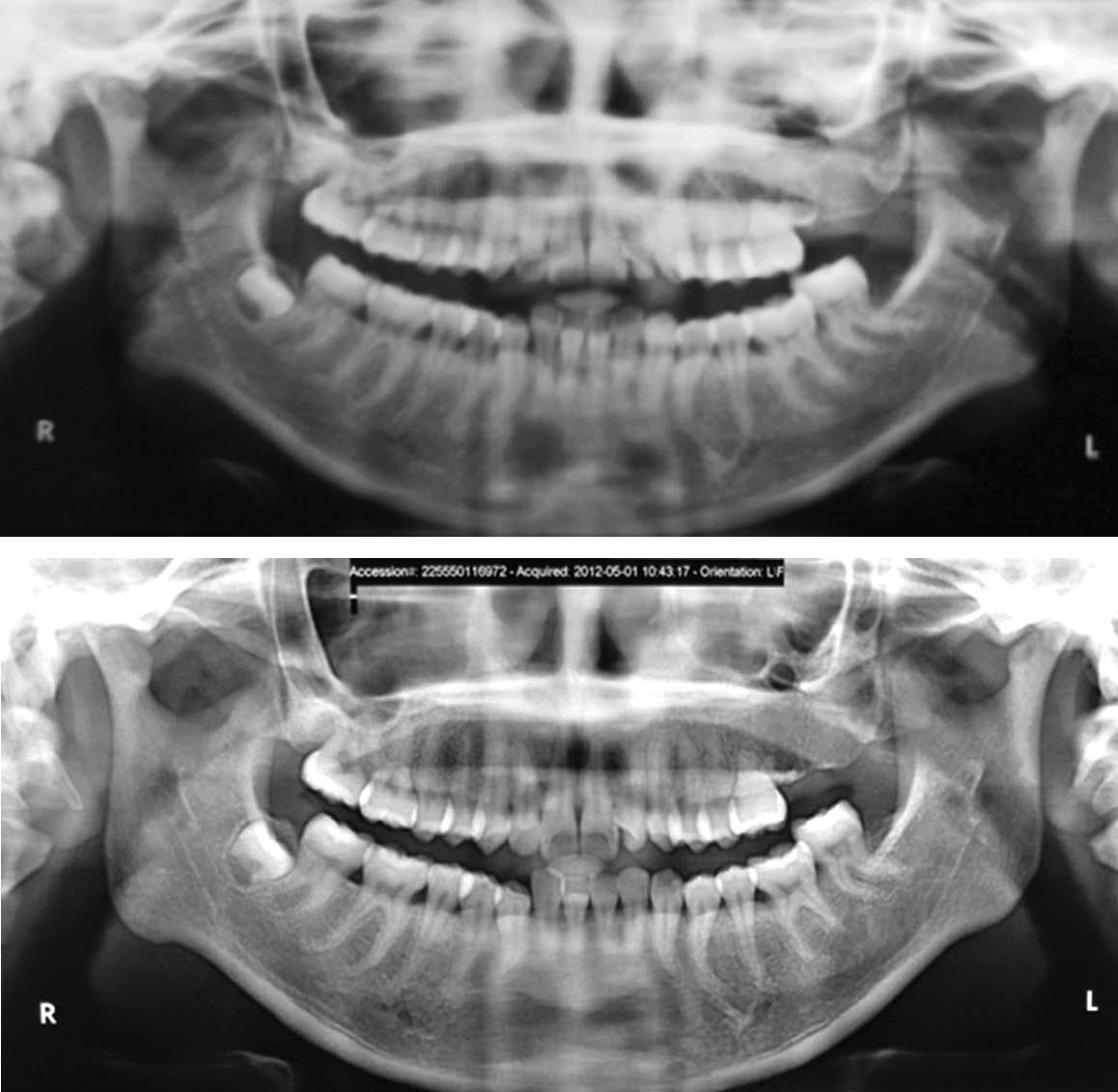
An unusual case of a large complex odontoma associated with unerupted maxillary molar of a 16-year-old Thai female patient is reported. This patient had no symptoms apart from a non-remarkable swelling at the left upper jaw bone. The lesion was accidentally detected during a radiographic investigation prior to orthodontic treatment. Upon clinical examination, the left upper second and third molars were absent. She had a bony hard swelling on the buccal and palatal sides of the left maxillary region without tenderness. The overlying mucosa appeared normal. The radiographic study revealed a homogeneous radiopaque mass at the left maxilla involving the maxillary sinus with a displaced molar tooth. This lesion was surgically removed after the histopathologic report confirmed it to be an odontoma. The result of treatment was satisfactory at the following check-up. The details of the treatment of this odontogenic tumor, and the literature reviewed, are discussed.
complex odontoma, maxillary sinus, unerupted tooth
10.31524/bkkmedj.2015.02.011